Why so BRASH? Prompt Recognition of an Uncommon Syndrome

“BRASH Syndrome is a somewhat newly described condition, with the acronym referring to Bradycardia, Renal Failure, AV Node Blockade, Shock and Hyperkalemia…”
Figure 1: patient’s EKG upon arrival to the ED
CASE
A 90-year-old male with a complex cardiac history including coronary artery disease s/p coronary artery bypass grafting, congestive heart failure (Ejection Fraction 45%), hypertension, and bilateral carotid artery stenosis, presents to the ED following an episode of loss of consciousness. Per patient’s wife, he patient became pale at home and subsequently dropped to the ground. After failing to awaken, the patient’s wife called 911 and began CPR. He has no history of seizures or syncope, and had not reported recent episodes of chest pain or shortness of breath to his family.
Upon EMS arrival, the patient was noted to have a weak pulse with associated bradycardia to 34 beats per minute (bpm). One milligram of atropine was subsequently administered, which briefly brought the patient’s heart rate to 90 bpm.
In the ED, the patient’s vitals were notable for bradycardia at 46 bpm and a blood pressure of 107/53 but were otherwise unremarkable.
EXAM
Constitutional: Ill-appearing
HEENT: mucous membranes moist, pupils equally round and reactive to light, eyes sluggish
Cardiovascular: bradycardic, regular rhythm
Pulmonary: normal effort, normal breath sounds
Abdominal: flat, nondistended
Skin: cool, pale
Neurological: unresponsive, Glasgow Coma Scale 4 (E1V1M4)
ABNORMAL/NOTABLE LABS
CBC: WBC (17.2), Hgb (10.0), Platelets (227)
BMP: Glucose (145), BUN (26), Creatinine (1.64), Sodium (135), Potassium (6.1)
High-Sensitivity Troponin: 22 -> 240 -> 1171
BNP: 563.6
DIAGNOSIS
BRASH Syndrome
DISCUSSION
BRASH Syndrome is a somewhat newly described condition, with the acronym referring to Bradycardia, Renal Failure, AV Node Blockade, Shock and Hyperkalemia (Figure 2). In the majority of patients, only severe hyperkalemia (often >7.0 mEq/L) or supratherapeutic doses of AV nodal blocking agents (such as beta blockers or calcium channel blockers) lead to clinically significant bradycardia. However, there is a synergistic effect between these two entities, where even mild hyperkalemia in patients on AV nodal blocking agents (particularly those renally cleared such as atenolol) can precipitate profound bradycardia [1]. This can subsequently initiate a vicious cycle stemming from decreased cardiac output. It is vital to identify this syndrome, as it can rapidly lead to multi-organ failure and hemodynamic instability.
The exact epidemiology of the syndrome is unknown, but is presumed to be underdiagnosed due to a lack of recognition [2]. It is speculated that BRASH will increase in frequency as the general population continues to age, in part due to compounding comorbidities. Increasing use of AV nodal blocking agents in the general population to combat atrial fibrillation and to abide by continuously stricter chronic hypertension guidelines also contributes to the rise in incidence.

Figure 2: BRASH Syndrome. https://litfl.com/brash-syndrome/
PATHOPHYSIOLOGY
The cycle of BRASH is ultimately driven by an underlying decrease in cardiac output, which can be calculated by multiplying the stroke volume by heart rate (Figure 3). The human body attempts to compensate for bradycardia with an increased diastolic filling time and subsequent increase in stroke volume. However, diastolic filling can only increase to an extent, and profound bradycardias will lead to poor perfusion, particualrly poor renal perfusion. The ensuing kidney damage decreases the clearance of potassium, worsening underlying hyperkalemia and continuing the cycle of BRASH. Hyperkalemia directly leads to bradycardia by reducing the resting membrane potential, which decreases the rate of action potential through the myocardium [3]. ACE-Inhibitors and ARBs can exacerbate this cycle by compounding both kidney injury and hyperkalemia.
In response to decreased cardiac output, the body attempts to maintain adequate mean arterial pressures by increasing peripheral resistance. It is imperative to comprehend and recognize occult shock, as patients may be underperfusing vital organs while maintaining an, ‘adequate’ blood pressure. Signs of hypoperfusion in the body include decreased urine output or cold extremities.
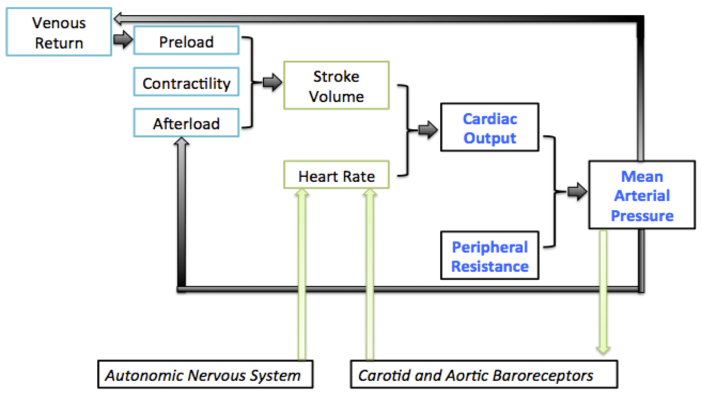
Figure 3: Adopted from MR Starling: Physiology of myocardial contraction, in Atlas of Heart Failure: Cardiac Function and Dysfunction, 3rd ed, WS Colucci and E Braundwald (eds). Current Medicine, 2002, p. 19-35
EVALUATION/TREATMENT
The clinical presentation of BRASH is highly variable and dependent on the degree of kidney dysfunction. Some patients may have underlying asymptomatic bradycardia, whereas end-stage BRASH can lead to full cardiogenic shock. The initial examination should evaluate for hemodynamic instability, as this will drive treatment options. In addition to physical examination, the precipitating factor of the patient’s bradycardia should be further evaluated through medication lists to assess for drug interactions or any recent dose changes, labs (with particular emphasis on electrolyte abnormalities), and EKG. The most important aspect of evaluating a bradycardic EKG is rhythm assessment, looking for junctional rhythms, or AV blocks. Additional assessment of the EKG for ischemic or hyperkalemic changes may help drive treatment options. It should be noted, however, that EKGs in BRASH patients are typically underwhelming; it is uncommon to see the stereotypical peaked T waves or QRS widening observed in isolated hyperkalemia.
In patients presenting with extreme bradycardia and hypotension, the diagnosis of BRASH may not be initially obvious. Initial treatment in these patients should be tailored to increasing the patient’s heart rate, which includes medical treatment and/or electrical pacing (Figure 4). As the underlying cause of the bradycardia in patients with BRASH is not vagally mediated, atropine will likely be unsuccessful.
The treatment of a stable BRASH patient focuses on lowering potassium levels and decreasing the concentration of AV blocking agents. Calcium should be initiated quickly to stabilize the cardiac membrane. An attempt should be made to temporarily drive potassium into the cells, often done through the use of insulin or beta agonists such as albuterol. In order to definitively remove potassium from the body, loop diuretics or gastrointestinal cation exchangers are typically used. Unless necessary, the patient’s AV blocking agents should be held. Dialysis may be required to remove these agents or to help lower significantly elevated potassium levels.
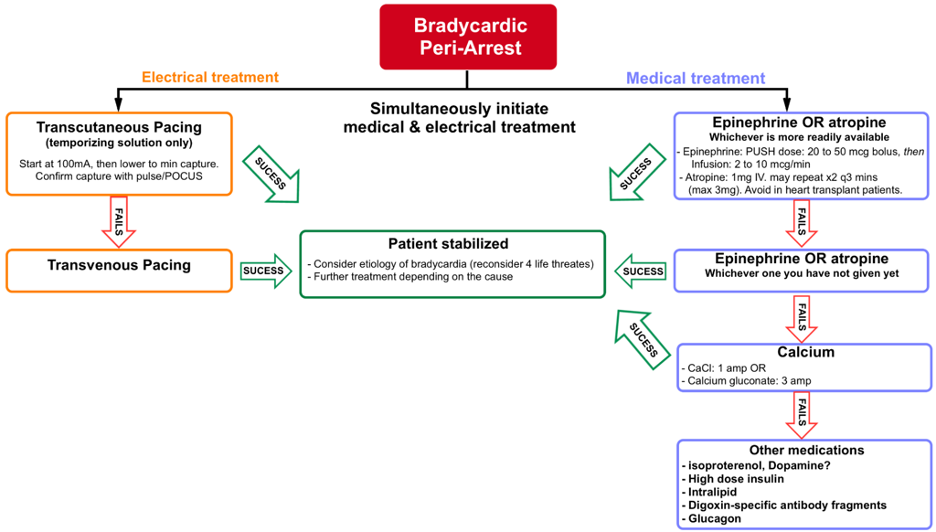
Figure 4: Flowchart of Bradycardic Peri-Arrest Treatment. https://recapem.com/evaluation-and-management-of-acute-unstable-bradycardia/
CASE RESOLUTION
The patient was subsequently admitted to the ICU, where he was evaluated by cardiology. His mental status and hemodynamics gradually improved after stopping his Metoprolol, Valsartan and Spironolactone, in addition to the direct treatment of his hyperkalemia. The patient received calcium, insulin/dextrose, furosemide and Lokelma while in the ICU. He did not require any pacing during his stay and was ultimately discharged on day 5 with a Holter monitor and prompt follow-up with his cardiologist.
AUTHOR: J. Kyle Volpe, MD, is a fouth year emergency medicine resident at Brown Emergency Medicine
FACULTY REVIEWER: Kristina McAteer, MD, is an attending physician and Rhode Island Hospital and Newport Hospital.
References
1. Saini, T., Reny, J., Hennawi, H. A., Cox, A., Janga, C., DeLiana, D., & McCaffrey, J. (2023, January 30). The vicious cycle of brash syndrome: A case report. Global cardiology science & practice. Retrieved April 23, 2023.
2. Lizyness K, Dewald O. Brash Syndrome [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (Fl): StatPearls Publishing; 2023 Jan-.
3. Hanumanthu BKJ, Chugh Y, Grushko M, Faillace RT. Hyperkalemia Presenting as Sinus Bradycardia, Junctional Rhythm and Atrial Bigeminy. Cureus. 2019 Dec 21;11(12):e6439. doi: 10.7759/cureus.6439. PMID: 31998568; PMCID: PMC6973538.