From Slip on Skateboard to Slip of Femoral Head: A Case of Pediatric Slipped Capital Femoral Epiphysis

…up to half of patients can present with knee pain, therefore SCFE should always be included in the differential diagnosis of pediatric patients presenting with knee pain…
Case
A 12-year old previously healthy male presents to the emergency department with right hip pain after falling from a skateboard two weeks prior. The pain has progressively worsened, is exacerbated by movement and weight-bearing, and alleviated with rest. The patient has been limping with ambulation and notes associated right knee pain. Family history is significant for a sibling with slipped capital femoral epiphysis (SCFE). Vitals were notable for a body mass index (BMI) of 32.8 (99th percentile for age and sex).
Vitals
BMI 32.8 | BP 118/75 mmHg | Pulse 85 beats per minute | Temperature 97.3F (36.3C) | Respiratory rate 20 breaths per minute | SpO2 100% on room air
Pertinent Exam
Patient in no acute distress, lying in bed with right lower extremity held in slight external rotation. Right hip and lower extremity non-tender to palpation. No edema of the right lower extremity. No warmth or swelling of the right hip or knee. Active and passive range of motion of the right hip is limited secondary to pain. No knee joint laxity. Strength and sensation of the right lower extremity intact. Palpable dorsalis pedis and posterior tibial pulses. Normal capillary refill of right lower extremity. Unremarkable examination of left lower extremity. Remainder of exam was within normal limits.
Imaging
Radiographs of right pelvis, hip, and femur consistent with bilateral SCFE. No radiographic abnormality of right knee.
Diagnosis
Bilateral slipped capital femoral epiphysis
Discussion
SCFE is a pediatric condition in which the femoral epiphysis (what will later become the femoral head) “slips” from its location on the growth plate. The direction of slipping is most often posteriorly and inferiorly in relation to the growth plate, also called the femoral physis, and the metaphysis. The slipped appearance on x-ray is often compared to a scoop of ice cream sliding off a cone.
SCFE often presents with hip, thigh, and/or groin pain. Importantly, up to half of patients can present with knee pain, therefore SCFE should always be included in the differential diagnosis of pediatric patients presenting with knee pain. Patients with SCFE will often experience pain with weightbearing and may ambulate with a limp. As with all chief complaints seen in the emergency department, a broad differential should be considered, including septic arthritis, Leg-Calve-Perthes disease, transient synovitis, fractures, osteomyelitis, and malignancy.
SCFE occurs most commonly in adolescent males with elevated BMI however it is also seen in adolescent females (male: female ratio 2:1.4). Of note, SCFE is the most common disorder of the hip in adolescence and can occur both in the presence or absence of a traumatic injury. While SCFE can be incited by trauma, it more commonly develops over a period of time, particularly during periods of growth such as puberty. Therefore, patients can present with pain that is acute or chronic.
The average age of presentation varies slightly for males and females with the average age of presentation in males being 12-13 years old and females being 11-12 years old. On average, SCFE can be present bilaterally in 25% of cases, therefore it is indicated to obtain bilateral hip imaging even in presentations of unilateral pain, as was seen in our patient. SCFE of the contralateral side can also present subsequently to the initial side, most often within 18 months. SCFE can also be a consequence of an underlying endocrine disorder such as hypothyroidism, hyperthyroidism, panhypopituitarism, or renal osteodystrophy. Therefore, workup of these endocrine disorders should be considered for patients presenting with SCFE who are younger than 10 years of age or less than 10-50th percentile for weight/height per one source, however specific criteria for which patients should undergo further workup varied by source.
SCFE can be classified as stable versus unstable based on weightbearing status with a non-weightbearing patient being considered to have an unstable SCFE. SCFE can also classified by the degree of difference in the angle between the epiphysis and diaphysis on the affected and unaffected hips via the Southwick Head Shaft Angle classifications of mild (<30 degree difference between sides), moderate (31-50 degree difference between sides), and severe (>50 degree difference between sides). In cases of bilateral SCFE, a reference degree is used. SCFE can also be graded by percentage of slippage into grades I, II, and III, with grade III reflecting the highest percentage of slippage.
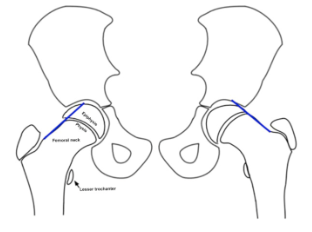
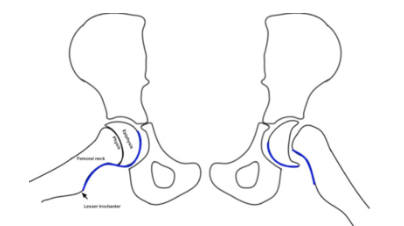
When SCFE is suspected, anterior posterior (AP) and frog-leg radiographs should be obtained. There are several radiographic findings used to diagnose SCFE including Klein’s Line and the “S” sign. Klein’s line can be visualized by drawing a line extending from the superior femoral neck on an AP x-ray. In a case of SCFE, this line will cross through less of the epiphysis than normal due to the slippage that has occurred. An example can be seen in the first illustration below. The “S” sign can be visualized by drawing a line along the inferior border of the femur up along the femoral neck and epiphysis on a frog leg x-ray. If this smooth “S” is disrupted, this is indicative of SCFE. An example can be seen in the second illustration below. A radiographic example of a right-sided SCFE can also be seen on the radiograph below. If radiographs are unrevealing and clinical suspicion for SCFE is high, MRI should be considered.
Example of Klein’s Line (abnormal on patient’s left side)
Source: Rebich EJ, Lee SS, Schlechter JA. The S Sign: A New Radiographic Tool to Aid in the Diagnosis of Slipped Capital Femoral Epiphysis. J Emerg Med. 2018 Jun;54(6):835-843. doi: 10.1016/j.jemermed.2018.01.023. Epub 2018 Mar 15. PMID: 29550284. Photos of Klein sign and S sign.
Example of “S” Sign (abnormal on patient’s left side)
Source: Rebich EJ, Lee SS, Schlechter JA. The S Sign: A New Radiographic Tool to Aid in the Diagnosis of Slipped Capital Femoral Epiphysis. J Emerg Med. 2018 Jun;54(6):835-843. doi: 10.1016/j.jemermed.2018.01.023. Epub 2018 Mar 15. PMID: 29550284. Photos of Klein sign and S sign.
Radiographic example of a right-sided SCFE

Source: Rebich EJ, Lee SS, Schlechter JA. The S Sign: A New Radiographic Tool to Aid in the Diagnosis of Slipped Capital Femoral Epiphysis. J Emerg Med. 2018 Jun;54(6):835-843. doi: 10.1016/j.jemermed.2018.01.023. Epub 2018 Mar 15. PMID: 29550284. Photos of Klein sign and S sign.
Once a diagnosis of SCFE is made, the patient should be made non-weightbearing and orthopedic surgery should be consulted. The patient should be admitted to the hospital. Definitive treatment of SCFE is surgical fixation. In some cases, prophylactic fixation of the contralateral side is performed. Complications of SCFE include but are not limited to arthritis, femoroacetabular impingement, cartilage loss, labral tear, leg-length discrepancy, and avascular necrosis.
Case Resolution
The patient was admitted to the orthopedics service, made non-weightbearing, and underwent bilateral in situ pinning. The patient did well post-operatively and was ultimately discharged home after working with physical therapy.
Take-Aways
SCFE is most commonly seen in adolescent males with elevated BMI
SCFE often presents with hip, thigh, and/or groin pain however up to half of patients can present with knee pain
While SCFE can be seen after trauma, it most often develops over a period of time and can therefore present as acute pain, chronic pain, or a combination
SCFE can be present bilaterally in 25% of cases, therefore it is indicated to obtain bilateral hip imaging even in presentations of unilateral pain
Radiographic findings used to diagnose SCFE include Klein’s Line and the “S” sign
Treatment of SCFE is operative fixation
Complications of SCFE include but are not limited to arthritis, femoroacetabular impingement, cartilage loss, labral tear, leg-length discrepancy, and avascular necrosis.
Keywords and Categories
Slipped Capital Femoral Epiphysis
SCFE
Pediatric hip and knee pain
References
Myers D, Souder C, Shirley E. Slipped Capital Femoral Epiphysis (SCFE). Orthobullets. Accessed at: https://www.orthobullets.com/pediatrics/4040/slipped-capital-femoral-epiphysis-scfe. Last updated February 3, 2025.
Ortho Info, American Academy of Orthopaedic Surgeons. Slipped Capital Femoral Epiphysis. Accessed at: https://orthoinfo.aaos.org/en/diseases--conditions/slipped-capital-femoral-epiphysis-scfe
Rebich EJ, Lee SS, Schlechter JA. The S Sign: A New Radiographic Tool to Aid in the Diagnosis of Slipped Capital Femoral Epiphysis. J Emerg Med. 2018 Jun;54(6):835-843. doi: 10.1016/j.jemermed.2018.01.023. Epub 2018 Mar 15. PMID: 29550284. Photos of Klein sign and S sign.
Sucato, Daniel J. MD, MS. Approach to the Hip for SCFE: The North American Perspective. Journal of Pediatric Orthopaedics 38():p S5-S12, July 2018. | DOI: 10.1097/BPO.0000000000001183
Webb CW, Liu R, Bouchereau-Lal N. Slipped Capital Femoral Epiphysis: Rapid Evidence Review. Am Fam Physician. 2025 Oct;112(4):414-423. PMID: 41118186.
Author
Kelsey Harper, MD is a fourth-year emergency medicine resident at Brown University Health/Rhode Island Hospital.
Faculty Reviewer
Meghan Beucher, MD Assistant Professor, Emergency Medicine & Pediatrics, Clinician Educator
Resident reviewer
Maggie Stark, DO, MS is a third-year emergency medicine resident at Brown University Health/Rhode Island Hospital.