BrownSound: Foreign Bodies
CASE
A resident is scrolling the electronic medical record and notices a new patient that just got roomed with the chief complaint “foreign body.” She thinks, foreign bodies always come with a story. I wonder what happened. She goes to see the patient, a 27 year old male with no past medical history who spent the afternoon surfing. He was walking back to his car barefoot and stepped on something that made him jump. He has no idea what it could be but “it’s still in there doc!” The resident takes a look at the bottom of his left foot and sees a small puncture wound over his heel but no palpable foreign body.
The resident thinks to herself I could x-ray his foot but so many foreign bodies are radiolucent and won’t be visible on xray. What if it’s a piece of shell, or glass? I could start digging at the site of the puncture wound to identify a foreign body, but what if there is nothing to find, and I cause more harm than benefit?
She decides that ultrasound is the best tool for this situation and a bedside point of care ultrasound is performed.

Figure 1: Linear hyperechoic area without acoustic shadowing
DIAGNOSIS
Soft Tissue Foreign body.
DISCUSSION
Radiopaque objects such as metal will likely appear on plain films, however objects made of wood or other organic material are radiolucent.
The user will want to start with the high-frequency (7.5-MHz or higher) linear array transducer that is usually used for soft tissue ultrasound. Apply gel and gently place the probe perpendicular to the skin where the patient is complaining of a foreign body sensation or pain. Alternatively, if there is significant discomfort with direct probe contact, the user can submerge the body part in a water bath, which serves as an excellent conduction medium for sound waves, and no direct contact with the tender skin is required.

Figure 2: Water bath used as an alternative to direct skin contact in foreign body identification. (http://www.emdocs.net/wp-content/uploads/2017/08/old-water-bath.png)
If the foreign body is glass an X-ray will often show the object (85% rate of detection [1]). However, that rate declines rapidly if the piece of glass is less than 2 mm in size [2]. This is where ultrasound can help. On an ultrasound, glass will appear hyperechoic with posterior shadowing. There will also often be a reverberation artifact (see comet tail before). If it has been present for greater than 24 hours, there may be a hypoechoic ring around it which would represent granulation tissue.

Figure 3: Glass (black arrows) in the soft tissue of a phalanx (from https://radiopaedia.org/articles/glass-foreign-bodies)
If the foreign body is wood or other organic material, it will appear echogenic and may cause posterior acoustic shadowing [3]

Figure 4: wooden splinter (between pointers) in a heel (from: https://radiopaedia.org/cases/foreign-body-in-heel-1?lang=us)

Figure 5: Thorn (between black arrows) in a scalp (https://radiopaedia.org/cases/foreign-body-scalp?lang=us)
If the foreign body is metal it will appear hyperechoic with posterior acoustic shadowing. With color flow Doppler, you may see a twinkling artifact. [4] Comet-tail artifact is common; which is a special form of reverberation artifact seen off of highly reflective objects such as glass or metal.
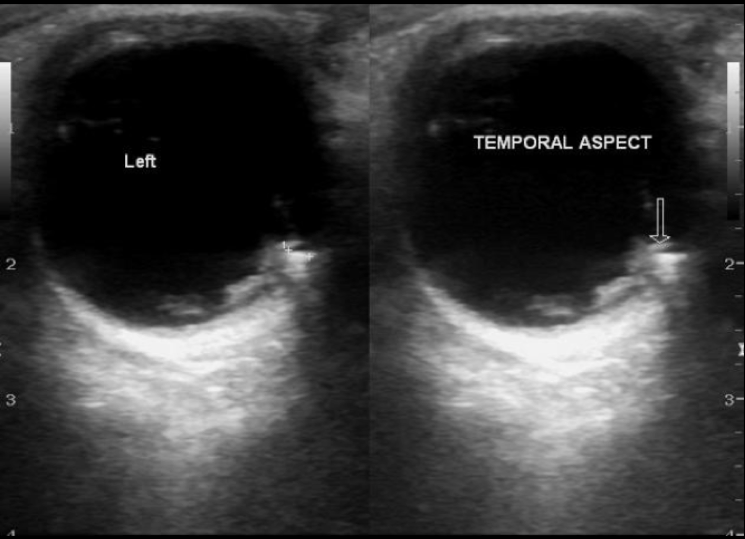
Figure 6: Periorbital metal foreign body (marked by black arrow) (https://radiopaedia.org/articles/ocular-foreign-body?lang=us)

Figure 7: Comet-tail artifact (labeled behind the foreign body which is highlighted by the single white arrow) (from https://www.acep.org/sonoguide/FB-Figure2.html)
If it’s a plastic foreign body, it would likely not be seen on x-ray but would appear hyperechoic on ultrasound with significant posterior shadowing [5] (think about what happens when you accidentally probe over an EKG electrode during a cardiac exam).

Figure 8: plastic (white arrows) with posterior shadowing (black arrow head) – (from https://www.ajronline.org/doi/full/10.2214/ajr.176.5.1761155)
![Figure 8: sand in soft tissue (between arrows) [6]](https://images.squarespace-cdn.com/content/v1/56e8a86a746fb97ea9d14740/1614969628244-HCUNFVABDYEJDISXNLHA/sand+.png)
Figure 8: sand in soft tissue (between arrows) [6]
CASE RESOLUTION
In this case, a hyperechoic foreign body with posterior shadowing was identified on ultrasound. After anesthetic was applied, a small incision was made in the skin that allowed for easy removal. The object was a small wooden splinter. Ultrasound was then used to assess and there was no remaining material so the patient was discharged.
TAKE-AWAYS
Ultrasound can be a resident’s best friend when trying to locate foreign bodies in soft tissue and unless they have concern for an underlying fracture, there may be no reason to order an x-ray. Finding a foreign body on ultrasound can also help them plan out their tactic for removal by telling them what the object could be, how deep it is, and in what plane the object lies.

{kind=link}
Author: Fahad Ali, MD 1st year Emergency Medicine Resident, Brown University
Faculty Reviewer: Kristin Dwyer, MD MPH, Assistant Professor Brown University, Director of Emergency Ultrasound Division, Director Emergency Ultrasound Fellowship.
References:
Cambridge textbook of accident and emergency medicine. Cambridge University Press. ISBN:0521433797.
2. Hunter T, Taljanovic M. Radiographics. 2003;23 (3): . doi:10.1148/rg.233025137
Boyse, Tedric D., et al. "US of soft-tissue foreign bodies and associated complications with surgical correlation." Radiographics 21.5 (2001): 1251-1256.
O. John Ma, James Mateer, Robert F. Reardon, Scott A. Joing. Ma and Mateer's Emergency Ultrasound, Third Edition. (2013) ISBN: 9780071793155
Horton, L. Kimberlee, et al. "Sonography and radiography of soft-tissue foreign bodies." American Journal of Roentgenology 176.5 (2001): 1155-1159.
Kaewlai, Rathachai, et al. "Imaging in tsunami trauma." Journal of Medical Ultrasound 17.1 (2009): 1-8.