Asynchrony PEM: Pediatric Gonadal Emergencies
Today, we’re talking gonads! Specifically, painful pediatric gonadal emergencies.
Gonadal emergencies present in the pediatric emergency department so many different ways; it's not as straightforward as kids complaining of testicular swelling or 'my ovaries hurt'. They usually present as pediatric abdominal pain. And because both that chief complaint and gonadal emergencies in general can cause you and your patient to cry, here's this week's theme song:
Kicking things off: Twist and Shout?
From our friends in Cincinnati, some key history and physical tips for your pediatric patients complaining of testicular pain. Important questions that our urology colleagues will ask about the physical exam include symmetry, testicular lie, and, most importantly, is there a cremasteric reflex? This was found to be 83.3% accurate in a 2004 study by Paul et al.
Citation: http://pemcincinnati.com/blog/pppp1/
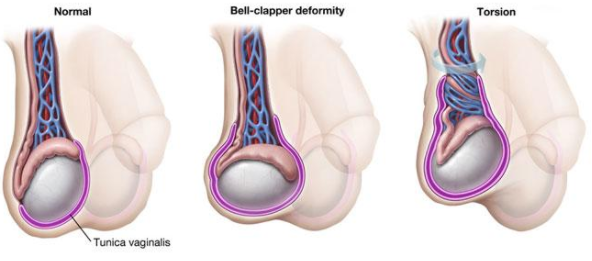
Patients with the bell-clapper deformity (a horizontal lie due to a defect in posterior attachment) are at an increased risk for torsion, based on the testicular lie.
What is your differential for pediatric testicular pain? More from our friends in Cincinnati: The emergency, the painful, and the treat or not to treat? And if you want more info on appendix testis torsion, or epididymitis PEDS EM Morsels has some brief input to check out.
But what if your patient has ovaries and not testicles?
These patients will present with acute onset abdominal pain, unilateral, and constant. Depending on how long the ovary has been twisted, pain can subside and become dull and mimic many different abdominal presentations, which is why it is often missed!
Ultrasound is not 100% in diagnosis and if you have high clinical suspicion, please call the urologists. Remember to ask our radiology colleagues to comment on the spermatic cord and flow in their report. And ask nicely!
Testicular torsion can even happy perinatally (no age is safe!). Check half way down the page for some quick tidbits on perinatal torsion. Check here for more information, but, in summary, testicular torsion can happen any time prenatally after the 6th week of gestation (when gonads form) to just before, during and after birth. Depending on when the torsion occurs, the infant might present with just a dusky hemiscrotum, firm hemiscrotum, or may just be an inconsolable infant.
But the gonads can do more that just twist, right? You betcha.
For the auditory learners listen to this quick (<10 minutes) podcast on ruptured ovarian cysts. (Note, we will not do transvaginal ultrasounds at Hasbro hospital, our home institution.)

Teenagers are also sexually active. Make sure to talk to patients about pregnancy, get a urine or serum b-HCG, and screen for PID. The American Academy of Pediatrics has guidelines for screening for STIs in adolescents. Basically: screen for gonorrhea, chlamydia, trichomoniasis, and syphilis as indicated. Don’t forget oral and anal swabs, as teens will have oral, vaginal, or anal sex.
And finally some Y chromosome specifics for when your patient gets their penis caught in a zipper or suffers from summer penile syndrome (for audio learners and readers).
That's it! Now you're ready to grab any gonadal emergency by the...horns.
See you next time in Asynchrony PEM!