The Obtunded Patient

“…came back from a walk and per family was ataxic, dysarthric and confused…”
The Case
52 y/o male with HTN, hyperlipidemia, chronic back pain, and recent depression came back from a walk and per family was ataxic, dysarthric and confused, so his family drove him to the ED. On the way, he began vomiting repeatedly and became increasing obtunded. As he entered the ED went into apparent cardiovascular and respiratory collapse. Given 2mg of Naloxone without response and intubated by RSI for further evaluation.
Examination
Vitals on arrival in the ED: Temp: 36, RR:-no spontaneous breaths noted after entering the ED O2: 88% on bag valve mask, HR: 68 BP: 88/64. Glucose 104. GCS 3 (non verbal, no motor movement, pupils 2mm and fixed). No corneal or occulacephalic reflexes noted, no cough or gag elicited. All extremities were flaccid and areflexic. EKG show sinus rhythm, no obvious conduction abnormalities.
Medication hx: Simvastatin 40 mg daily, amlodipine 10 mg daily, Baclofen 20 mg TID, Vicodin 5-300 1 tablet q6 hrs
Labs: ETOH: 150. CBC, lactic acid, chemistry, venous blood gas (on ventilator), CPK, LFT’s, troponin asa, acetaminophen, UA, UDS all WNL
Imaging: CTA pan scan negative except for mild aspiration in the R lung base.
So what happened…..?
What is it?

Baclofen is a synthetic derivative of the naturally occurring inhibitory neurotransmitter GABA.
Acts principally on the GABA-B receptor at the spinal level and reduce the post-synaptic potentials along motor neurons, thus relaxing the skeletal muscles.
Baclofen is primarily used for the treatment of spastic movement disorders and now more ubiquitously for the treatment of chronic back pain.
How is it given?
Oral: Until the past 10 years, the primary method of administration of Baclofen was oral.
Peak concentration in 2 hours and half life of 3.5hours
Dosage 40-80mg daily dosed q8 hrs
Centrally acting but crosses the blood brain barrier ineffectively, limiting its bioavailability
Very low toxic range with severe toxicity from oral baclofen, necessitating ICU level care occurring fairly consistently with baclofen overdoses of over 200mg (a 3 day supply for most people)
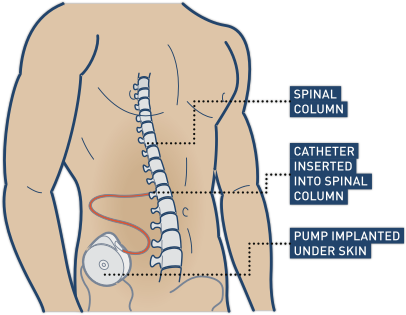
Figure 2: Baclofen pump concept
Intrathecal: Intrathecal baclofen is administered through the implantation of a pump subcutaneously with a catheter from the pump inserted directly into the CSF fluid.
Dosage: 90 mcg to 800 mcg daily
Intrathecal baclofen allows for 4x the amount of baclofen to be delivered to the spinal cord with just 1% of the oral dose.
Intrathecal Baclofen Pumps: The pump is surgically implanted under the skin in the abdomen and the catheter is tunneled under the skin and inserted into the intrathecal space usually between the 1st and 2nd lumbar vertebrae.
Currently SynchroMed is the only pump currently being used in the US for intrathecal baclofen, hydromorphone and morphine
The catheter holds 3-4ml
The reservoir holds 20-40ml
Pump battery lasts for 5-7 years

Figure 3: Synchromed Baclofen pump
Toxicities
Baclofen has the potential for both overdose and withdrawal, which can both present with a wide array of symptoms.
Overdose Symptoms
Most commonly include CNS depression, lethargy, somnolence, hallucinations, agitation, mydriasis/miosis, nausea and vomiting
Severe toxicity is associated with bradycardia, hypotension (more common) or hypertension, respiratory failure, hypothermia, seizures, coma and death.
Rarely, rhabdomyolysis and conduction disturbances may occur
Causes
Oral Baclofen overdoses:
Usually intentional overdoses-either for recreational or self harm
Intrathecal baclofen overdoses:
Wrong dose is manually programmed into the pump
Wrong concentration is placed in the pump
Wrong bolus is given when starting the pump
Wrong port is accessed or wrong port filled
Treatment
Patients are usually treated by supportive methods only.
In severe overdoses, this often means supporting blood pressure with fluids and pressors and often-mechanical ventilation for respiratory failure until drug toxicity subsides.
Generally overdose symptoms will resolve in approximately 24-48 hours
For Intrathecal baclofen overdoses:
Most are correctable by emptying the pump reservoir:
Turn off pump-programmer (need external device programmer to do this)
Empty reservoir: Use a 22 gauge needle to stick the middle of the pump and pull out all the drug

Figure 4: Emptying the reservoir
Remove the CSF- Use a 24-25 gauge needle to stick the side port and aspirate 30-100 ml of CSF
In severe cases performing a lumbar puncture to reduce circulating baclofen in the CSF while performing all normal supportive strategies (small case reports- this involves replacing entire circulating volume of CSF with saline and has been used successfully in a few cases of massive overdose)

Withdrawal Symptoms
Similar to withdrawal from alcohol or benzodiazepines, with the loss of gaba-mediated inhibition: hyper metabolic states, spasticity/rigidity, hallucinations/seizures, tachycardia, hyperthermia, and hypertension are more commonly observed.
Mild: pruritus, agitation, diaphoresis and increased tone
Moderate: fever, tachycardia, spontaneous clonus and painful muscle spasm
Severe: worsening of above along with seizures, delirium, hallucinations, rhabdomyolysis and death.
Remember the mnemonic, "ITCHY, TWITCHY, BITCHY."
Causes of Withdrawal
Oral Baclofen Withdrawal:
Oral Baclofen withdrawal can occur when a person is abruptly stops taking baclofen or weans off to fast.
Of note oral baclofen diffuses through the blood brain barrier deep into the brain whereas- intrathecal baclofen stays almost exclusively in the CSF with a penetration of only approximately 1-2 inches into the brain. Therefore, a person who is being switched to intrathecal baclofen must still be tapered off their oral baclofen or they will withdraw.
Intrathecal Baclofen Withdrawal:
Intrathecal Pump Malfunction
Intrinsic pump malfunction is exceedingly rare.
Pocket Refill
Rather than an overdose this results in acute withdrawal as intrathecal dosing is 1/100th of oral dosing/subcutaneous dosing.
Battery failure
Expected to die at 84 months.
Will alarm 3 months prior.
Medication Changes or interactions:
SSRI’s especially known for decreasing effect
Catheter malfunctions: (kink, micro/macroleaks, scarring, migration)
Most common cause of pump failure
KUB and AP/lateral spine first step to look for catheter fracture or migration

Figure 6: KUB demonstrating Baclofen pump
Treatment
Oral Baclofen withdrawal is usually easily treatable by restarting baclofen and introducing a slow tapered wean if discontinuation is desired.
Intrathecal Baclofen Withdrawal presents more of a challenge in both recognition and treatment. It can be tricky to recognize baclofen withdrawal as it often masquerades as sepsis (ex-tachycardia, hyperthermia, altered mental status). It is important to recognize that many of these patients have severe spasticity and may have limited verbalization skills. Often they come from long term care facilities without much information, along with the fact that many times the baclofen will not be listed on their daily facility medication list, making it extremely important to look for a pump every time.
Recognizing that a patient’s symptoms may be secondary to intrathecal baclofen and interrogating the pump and obtaining pump series imaging to evaluate for catheter related malfunctions is a key first step
Essentially intrathecal baclofen withdrawal requires intrathecal baclofen. The key is finding the reason for the withdrawal and fixing the primary cause. Everything else is a temporizing measure.
To help with symptoms while attempting to fix the primary cause of pump failure treatment can include:
High Dose Oral Baclofen
Treating intrathecal baclofen withdrawal with oral baclofen is often unsuccessful as the vast difference in bioavailability of oral doses and intrathecal doses.
Benzodiazepine treatment
Propofol low dose
Experimentation with Dexamedetomidine and cyproheptadine
CSF infusion of Baclofen
So what happened to our patient?
After approximately 18 hours intubated, our patient began waking up, became agitated and self-extubated himself. He admitted to taking approximately 900 mg of baclofen in a suicide attempt the day of admission. He was discharged to inpatient psychiatry without any further medical sequela on hospital day 3.
Take Home Points
Overdose: variable presentation, CNS depression is often involved, good supportive care is key.
Withdrawal: variable presentation, Itchy/twitchy/bitchy. Will have increased muscle tone from baseline.
Always remember the pump is there.
Overdose: For intrathecal overdose-2 ports from which you can draw drug and CSF back out.
Withdrawal: Look for the cause and treat supportively with oral baclofen, benzos, and propofol.
Faculty Reviewer: Dr. Kristina McAteer
References
Image 1: “Spasticity2” by Bill Connelly- Own Work
https://commons.wikimedia.org/wiki/File:Spasticity2.svg
Image 2: http://www.gablofen.com/patients/intrathecal-baclofen-therapy
Image 3: http://www.ajnr.org/content/32/7/1158
Image 4: http://www.rch.org.au/kidsinfo/fact_sheets/Intrathecal_baclofen_3_the_ITB_pump/
Image 5: http://www.cliparthut.com/clip-arts/175/people-clip-art-175256.gif
Image 6: https://emcow.files.wordpress.com/2014/01/baclofen-3.jpg