A Tale of Two Bleeders
The following are two cases of vaginal bleeding seen in the a community Emergency Department during the same shift.
CASE 1:
HPI: 30 year old G3P1 female at 5 weeks pregnancy by LMP who presents to the ED with vaginal spotting. She states it started this morning while urinating. She reports about “a spoonful” of dark red blood with no clots. Associated symptoms include transient, lower abdominal cramping. Her pregnancy has had no complications so far, and she just established pre-natal care. Her second pregnancy was complicated by preterm delivery, for which she underwent C-section.
PE: Hemodynamically stable. No abdominal tenderness, guarding, rebound, or distention. On speculum exam, there is a mild amount of dark red blood and clot in the vaginal vault. No fetal tissue. The cervical os is closed. No CMT. No uterine or adnexal tenderness.
Bedside TVUS: No IUP
What now?
In any case of vaginal bleeding, the first step is determining if the patient is pregnant or not! In this case, we know our patient is pregnant. At this point, we develop our differential:
Ectopic Pregnancy
Abortion
Gestational trophoblastic disease
Implantation bleeding
Unlike our Miranda Rights, your patient is guilty of ectopic pregnancy until proven innocent! This is one of the “can’t-miss” diagnoses that we should all feel comfortable working up and managing.
Ectopic Pregnancy:
This occurs when there is conception outside of the uterine cavity. Risk factors include a history of STIs (especially PID), assisted reproductive techniques, history of pelvic surgery, advanced maternal age, previous ectopic pregnancy, and cigarette smoking.
The vast majority of ectopics take place in the fallopian tubes (ampullary portion), with about 1% taking place in the abdominal cavity, and <1% are cervical.
Most patient’s report a history of missed menses, although up to 15% of patients will report normal menses.
Abdominal pain is present in up to 90% of patients with ectopic pregnancies (secondary to tubal distention or rupture), although the absence of pain does not rule out ectopic pregnancy!
The physical examination in ectopic pregnancy is variable. In cases of ruptured ectopic pregnancy, the patients may be peritoneal with adnexal tenderness and possibly present in shock. Most patients, however, present with stable vital signs. An adnexal mass or tenderness could be an ectopic, although can also be a corpus luteum cyst in the setting of normal pregnancy and/or recent ovulation. Blood may be appreciated in the vaginal vault, although pelvic examination may be normal as well.
Definitive diagnosis of ectopic pregnancy is by ultrasound or direct visualization during laparoscopy or surgery.
But what about the beta-HCG level? Although absolute levels and “doubling times” are typically longer in ectopic pregnancy, it turns out that no level can reliably distinguish between a normal and pathological pregnancy.
The literature describes a discriminatory zone, or beta-HCG level at which you would expect to see an IUP at 1,500 mIU/mL for transvaginal scanning and 6,000 mIU/mL for transabdominal scanning. That being said, if ectopic is suspected, ultrasound should still be performed even with low beta-HCG levels.
The goal of ultrasound is to locate a viable IUP and exclude ectopic pregnancy. Visualizing an IUP is reassuring, although does not definitively exclude ectopic pregnancy if the patient is at high risk for a heterotopic pregnancy. Heterotopic pregnancy (both IUP and ectopic) has increased in the general population, largely in the setting of assisted reproduction technology (currently about 1:3,000 pregnancies).
An empty uterus with an embryo visualized outside the uterus is diagnostic, however this is only seen in up to 10% of transabdominal scans, and up to 25% of transvaginal scans. A pelvic mass (especially adnexal) in the setting of free fluid (evaluated in the cul de sac, posterior to the uterus) is highly suggestive of ectopic pregnancy.
If an ultrasound is indeterminate and the patient is hemodynamically stable, the patient should have close OB/GYN follow up in two days for a repeat beta-HCG level and be given strict return precautions. However, if the patient’s beta-HCG was above the discriminatory zone, it is advisable to seek consultation in the ED prior to disposition.
For ruptured ectopic pregnancies, surgical treatment is the preferred treatment modality.
For unruptured ectopic pregnancies, in the absence of contraindications, patients who are hemodynamically stable with minimal symptoms and who have appropriate OB follow up, medical treatment with methotrexate can be considered. This is typically given as a single IM dose, although the success rate of a multiple dose regimen was shown to be higher (92.7% vs 88.1%, p<0.05).
Treatment failure overall occurs in about 1/3 of cases. There is about a 5% chance of ectopic rupture and patients should avoid sexual intercourse for 2-3 weeks given the risk for this.
Abdominal pain 3-7 days after treatment with methotrexate is a common side effect, often attributed to tubal abortion/distention, although is difficult to differentiate from treatment failure and ectopic rupture. It is suggested that these patients undergo repeat laboratory testing (CBC) and pelvic ultrasound.

Figure 1: Ectopic pregnancy within the left adnexae. Source: Radiopaedia.org
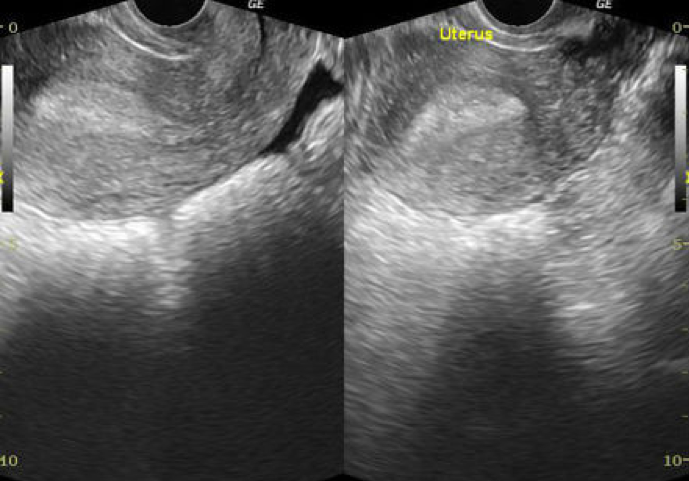
Figure 2: Fluid appreciated in the cul-de-sac posterior to the uterus. Source: Radiopaedia.org
CASE 2:
History: 36 year old female G3P2 s/p D&C for a missed abortion at 7 weeks who presents to the ED with three days of worsening vaginal bleeding. Today, she reports “a large amount” of dark, red blood with clots. She reports using a pad every 10-15 minutes. Associated symptoms include intermittent, lower abdominal cramping and fatigue. No other associated symptoms. No pregnancy complications in the past.
Pertinent PE: No abdominal tenderness, guarding, rebound, or distention. On speculum examination, there is a moderate amount of blood in the vaginal vault with clots. No fetal tissue. The cervical os is closed. No CMT. No adnexal or uterine tenderness.
Bedside TVUS: No IUP. Heterogenous material appreciated within the uterine cavity.
What now?
This is a case of a patient with retained products of conception (RPOC) following an abortion.
Patient’s will often present with vaginal bleeding and pelvic pain, which are expected symptoms typically associated with low morbidity.
In patients with heavy vaginal bleeding, prolonged bleeding greater than three weeks, fever, uterine tenderness, and/or pain not controlled by over the counter medications, further evaluation is indicated to rule out other potential etiologies (or rule in RPOC).
Ultrasound is the best imaging modality to assess for RPOC
In patients with RPOC and bleeding greater than three weeks, hemodynamic instability, or sepsis, surgical treatment is preferred.
Patients can otherwise opt for expectant management or medical management, which typically consists of a dose of misoprostol (intravaginally or oral), especially given its low cost, low side effect profile, and easy availability. Notably, after consultation with the patient’s OB/GYN, our patient went home on methergine (an ergot alkaloid and uterotonic medication).
And for both cases, don’t forget the rhogam for your Rh negative patients! The dose is generally 300 micrograms given IM.
Faculty Reviewer: Dr. Kristy McAteer
REFERENCES:
Carusi, Daniella et al. Retained Products of Conception. UptoDate. <www.uptodate.com>. 2018.
Ibrahim, Dalia, Gaillard, Frank, et al. Ectopic Pregnancy. Radiopaedia. <https://radiopaedia.org/articles/ectopic-pregnancy>. 2018.
Tintinalli, et. al. Ectopic Pregnancies and Emergencies in the First 20 Weeks of Pregnancy. Emergency Medicine. 8th Edition. 2016. 628-633.HHHf
FURTHER READING:
1st Trimester Pregnancy Ultrasound Podcast Part I: http://www.ultrasoundpodcast.com/2014/10/pregnancy-ultrasound-part-1-foamed-back-back-basics-cabo-update/
1st Trimester Pregnancy Ultrasound Podcast Part II: http://www.ultrasoundpodcast.com/2014/10/1st-trimester-pregnancy-ultrasound-part-2-ectopic-topics-foamed/
EM in 5: First Trimester Bleeding https://emin5.com/2015/11/09/vaginal-bleeding-in-1st-tm-pregnancy/
EM Updates: Ruling out Ectopic Pregnancy http://emupdates.com/2013/06/03/rule-out-ectopic-in-the-emergency-department/