Scalpel…Finger…Glock: Medical Support of Law Enforcement Tactical Teams
OVERVIEW
Over the last three decades, the spectrum of crime in the United States has posed a dynamic challenge to law enforcement, with an increasing prevalence of violent incidents involving assault weapons, domestic terrorism, and often mass casualties. To meet the demand of these emerging situations, law enforcement agencies have formed groups of officers with specialized equipment and training, capable of handling these unique threats affecting both law enforcement and the general public. Although these teams are branded differently (such as Special Response Teams, or Quick Reaction Teams), they are collectively referred to as Special Weapons and Tactics (SWAT) teams. The proliferation of SWAT teams has generated a rising need for specialized medical providers capable of supporting both the needs of these tactical operators, and assisting ill or injured patients/suspects encountered during tactical operations. Standard emergency medical care procedures frequently contradict the demands of the tactical environment, which is often dangerous or austere, leading to the advent of a specific field of prehospital care: Tactical EMS or TEMS.
This two-part post will first review the broad strokes of tactical EMS and the aspects of medical support required for most civilian law enforcement tactical teams, followed by specific details related to direct “hands-on” medical care in the tactical environment. Many of the points highlighted are presented by national tactical EMS courses, such as the Counter Narcotics and Terrorism Operational Medical Support (CONTOMS) course and the Tactical Combat Casualty Care/Tactical Emergency Casualty Care (TCCC/TECC) program, both of which serve as the foundation for most TEMS care provided in the U.S.
PART 1: Overview, Considerations, and Controversies
Background:
Current tactical medical care provided for civilian law enforcement is mostly adapted from military guidelines. Although battlefield medical care can be traced back to ancient Roman times, the framework of modern tactical medical support finds origins in the 1960s. [1] As U.S. soldiers encountered more unconventional warfare in Vietnam, special operations teams, such as the Navy SEALs, rose to meet this new challenge; [2] it was quickly realized that these select teams required customized medical support to meet the needs of prolonged, forward field care. Since then, the military has continued its robust specialized training for combat medics, including the elite Joint Special Operations Medical Training Center at Fort Bragg, N.C., furthering battlefield medical care and providing foundations for management of common traumatic injuries beyond the battleground. These military guidelines serve as an excellent core, but fundamental differences from the battlefield environment to the civilian realm, such as pattern of injury, rules of engagement, and treatment modalities, require specific delineation for civilian applications.
In August 1966, Charles Whitman climbed the clock tower at the University of Texas-Austin with an array of weapons, proceeding to rain terror on innocent victims below in what is often referred to as the first mass shooting incident. It took several armed officers and civilians nearly 96 minutes to end this threat, as coordinated response to such an incident had never been implemented previously. [5] Law enforcement agencies realized the importance of developing groups of officers with specialized training, equipment, and tactics to respond to these types of incidents, leading to the birth of SWAT teams. Mass shooting events in recent history, including the 1997 North Hollywood shootout, the Sandy Hook Elementary School incident, and the Las Vegas music festival incident, among others, continue to support the need for these teams, and their attached specialized medical components.
General Support Considerations:
Prior to initiating support for any law enforcement tactical team on an administrative, or operational level, medical providers need to understand some unique elements of team dynamics and medical care in this environment. Additionally, some controversial areas of support need to be considered and addressed, as not doing so can be a “make or break” decision.
Know your audience: Law enforcement, like other emergency services, is a particularly close knit group, following a para-military organizational structure. Officers are bonded by shared experiences in the police academy, and through challenging, sometimes life-altering cases in the performance of daily duties. This bond is further amplified in tactical teams, where providers spend significant time training for low frequency/high severity situations that necessitate inherent life or death trust on each other. Medical providers stepping into this role, even with previous pre-hospital, military, or law enforcement experience, need to be sensitive to this dynamic, and consider this in support elements. Often the easiest way to both show initiative and respect of this relationship is to commit face time to all aspects of team operations, which fosters mutual trust and understanding between all parties.
Shhhh…. Operational Security (OPSEC): Medical providers must understand the importance of OPSEC in support of tactical teams. Although the provisions of HIPAA and confidentiality are embedded in healthcare, security and confidentiality around tactical operations have a direct downstream effect to both mission success, and to the safety of operators in high risk cases. Providers will often be required to obtain background screening and security clearance, but need to be vigilant regarding tactics, operations, and training. Even a simple, inadvertent disclosure with the wrong individual about team tactics or upcoming operations can have catastrophic consequences to operator safety and mission success.
BSI…Scene Safety?: Provision of care in the tactical environment directly challenges many EMS care paradigms, particularly with regard to hostile environments, where standard training mandates providers “stage away” and await scene safety. Since the original supporting position statement from the National Tactical Officer’s Association in 1993, TEMS has garnered additional support from other national groups, including NAEMSP and ACEP. Through understanding of team tactics, as well as patterns of wounding frequently seen in mass-casualty shooting events, these position statements strongly advocate for a dedicated medical element close to team point of operations. Of note, many civilian agencies have adapted a Rescue Task Force model, pushing unarmed providers with dedicated protection and specialized equipment further to points of care in these incidents. While this is an important step in advancing care in mass-wounding events, it does not supersede the need for a dedicated tactical medical element for law enforcement operations.
Not So Fast: Controversial Decisions
Due to the unique nature of TEMS and more recent growth/acceptance in the law enforcement and first responder communities, several basic facets of TEMS care are often hotly debated, and can create significant controversy for both medical providers and law enforcement agencies. In addition to the general considerations above, depending on specific team operations, these areas should be carefully reviewed prior to commitment for tactical support. Many of these scenarios are well-highlighted in the CONTOMS Medical Director’s course for reference. [5]
The “Who” Question: The decision of who will actually provide “boots on the ground” support for a tactical team can be challenging. Although all medical care requires oversight by a physician medical director, actual care for team members can be supplied by a wide array of providers. Certain models employ direct physician support (such as Dallas Police SWAT), but other levels of healthcare providers, including RNs, PAs, paramedics, and EMTs can fulfill this role. Several aspects are to be considered when determining ideal care model, including cost, availability, and scope of practice. For example, a physician brings a wealth of experience, knowledge, and ability for field care to the table, but are an expensive asset, with limited availability due to clinical schedules. On the other end of the spectrum, EMTs are abundantly available, have strong basic medical skills, and tactical officers can be crossed-trained to this level for team support; nonetheless, some tactical medical care procedures/equipment are outside the scope of practice for basic EMTs and create challenges in the prolonged care scenario. To balance these, most teams will employ a tactical medical component somewhere in the middle (often paramedics with specialized training), but exactly who does this needs to be considered based upon resources and needs of a specific team.
The Firearm Question: An understanding of firearms and firearm safety is a non-negotiable element of tactical medical care, but arming of tactical medical providers is one of the most hotly debated topics in TEMS. Introduction of firearms adds layers regarding safety, legality, training, and liability. For non-deputized medical providers, this question raises the most concerns, including authorization of deadly force and associated legal protections, the ethical dilemma of engaging suspects and subsequent treatment, weapons safety/retention, that can be hard to rectify. A summary of pros and cons is listed below, modified from the CONTOMS Weapons Matrix. [5]

Table 1. Pros and Cons of Firearms
3. The Location Question: Determining ideal location for TEMS providers regardless of level of training is also hotly debated, and this does follow a progression from the discussion above about armed vs. unarmed providers. As mentioned above, most medical societies involved in TEMS care recommend a forward, dedicated element for law enforcement, as a standby EMS element alone is not sufficient. The ideal location will depend on several factors, and this is additionally well reviewed in the CONTOMS program: [5]
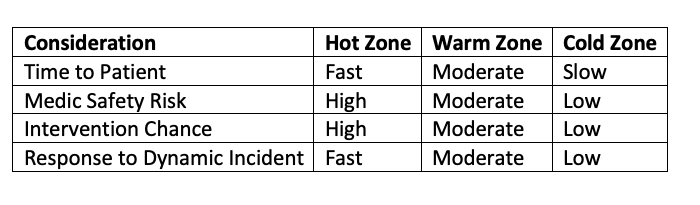
Table 2. Determining Ideal Location
4. The Role Question: Medical providers attached to a tactical team may be faced with a challenge of role confusion. For armed providers this is most challenging, as one can quickly shift from medical provider to threat suppression. Law enforcement agents with medical training and filling a TEMS role can be challenged by serving both roles as a dynamic incident unfolds. Ethical considerations are also brought forth, as medical providers can become torn between caring for team members, injured civilians, or injured suspects.
5. The “Not Talked About” Question: For a majority of medical providers supporting a tactical team, this will be done on a voluntary basis. Due to the potential for liability on several levels, it is important for a formal agreement to be in place, such as a Memorandum of Understanding (MOU). Particularly for medical directors, details about malpractice insurance and other liability insurance should be explicitly discussed; many law enforcement agencies do not primarily provide medical care, and incidents resulting in a malpractice claim may not be covered under existing policies. Additionally, insurance considerations such as disability coverage, and vehicle insurance coverage (if responding to a scene using a personal vehicle) should be explicitly reviewed prior to entering a formal agreement.
PART 2: Tactical Medical Care
In Part 2, we will discuss specific aspects of tactical medical care in support of law enforcement teams, including typical day-to-day operations and direct care during team deployment.
Tactical Medical Care:
When reviewing course offerings and material, a majority of focus is placed on specific tactical medical care protocols and procedures. Despite the importance of these discussed further below, a majority of medical care for tactical teams revolves around preparation/preparedness, and care for minor injuries or complaints.
“Hey Doc, I have a question…”: After medical providers build a strong relationship with tactical operators, team members may choose to seek “internal” care for common medical complaints or questions. For physician medical directors, regardless of trained specialty, operators may see the team physician as an ally and present for primary care considerations. Non-physician TEMS providers often have protocols in place to care for common complaints or injuries, such as wound care, that fall outside the normal prevue of EMS protocols, allowing the team to maintain constant readiness.
Check the Boxes: Beyond routine medical care, TEMS providers especially at the physician level may be called upon to assist with other support modalities for the team. This could include ongoing preparedness, such as nutrition or fitness plans, vaccines, or other “unspeakable” considerations like maintaining a repository of dental records or DNA in the event of a catastrophic injury.
Medical Threat Assessment (MTA): A critical component in pre-planning, this involves collection of medical intelligence critical to the operations of the team, often for a given operation. Depending on the operation and location, this can be straight-forward, with considerations such as immediate medical support, local receiving facilities, and EMS resources. On the contrary, prolonged or austere operations can require extensive considerations and pre-planning, including work/rest cycles, as well as specific equipment; this can be further understood using the two examples below:
a. Scenario 1: A SWAT team for a city agency in Rhode Island conducts their scheduled firearms/range training day. All officers have individual first-aid kits (IFAKs), there are designated primary and secondary medical providers, EMS response to the range averages 4 minutes, and there are two large hospitals, including a Level 1 trauma center within 15 minutes of the facility. The supporting medical director is on site for training, and familiar with the team and local hospital facilities, and completes a brief MTA form for the session.
b. Scenario 2: A covert tactical team for a federal law enforcement agency is planning a high risk warrant for a potential drug lab in rural Arizona. The supporting TEMS providers gather to plan a MTA for the operation. Unlike above, the team recognizes multiple complexities affecting the planned mission: ambient temperature is expected to be 100 degrees, several venomous animals are native to the region, the local community hospital is 15 minutes by ground, but the Level 1 trauma center is 150 miles away and helicopter EMS is limited. The team realizes they need to extensively plan, and put in place multiple contingencies to cover medical threats to the operators.
![Figure 1: A sample Medical Threat Assessment form provided through the CONTOMS program, covering just a portion of what medical providers must consider for a given training or operation[6]. ](https://images.squarespace-cdn.com/content/v1/56e8a86a746fb97ea9d14740/1621108078778-35V9P1JEP0SK4Q3ZUMHB/MTA+.png)
Figure 1: A sample Medical Threat Assessment form provided through the CONTOMS program, covering just a portion of what medical providers must consider for a given training or operation[6].
4. Sick Call: A specific subset of tactical medicine that facilitates health and safety of critical public safety personnel during training, high risk, or prolonged operations. TEMS providers can assist team members in keeping operators in the fight, by addressing common medical concerns, such as sprains or lacerations, without a trip to a hospital.
![Figure 2: A sample of some common medications carried in a sick-call formulary for TEMS providers, as presented by Dr. Ameen Jamali at the SOMA National Conference, 2018[7]. ](https://images.squarespace-cdn.com/content/v1/56e8a86a746fb97ea9d14740/1621108117161-HCH2Q0FNDP1IGBUKARLE/Sick+.png)
Figure 2: A sample of some common medications carried in a sick-call formulary for TEMS providers, as presented by Dr. Ameen Jamali at the SOMA National Conference, 2018[7].
5. Tactical Primary Survey:
Of the acute care performed in the tactical environment, the primary survey is of paramount importance. Although tenets of trauma care are mostly unchanged, there are some specific modifications to the tactical environment, meant to address specific injuries expected during operations. Depending on training, the approach to the primary survey can be presented slightly differently (XABCDE for CONTOMS, MARCH assessment for TCCC), but core elements of recognition and treatment are similar. The Committee on Tactical Combat Casualty Care maintains a list of recommended devices and adjuncts to be used in the tactical environment. [8]
a. First Things First: Before any acute care can be performed, providers need to ensure safety, by returning fire at a threat, and obtaining cover/concealment to perform a primary survey. For operators that are injured and can participate in self-care, encourage use of IFAK materials until medical care can be safely performed.
i. A critical consideration once a safe haven is reached is CLEARing a casualty: Confirm identity (friend/suspect), Look for weapons/devices, Ensure safe location (security), Acquire intelligence, and practice Retention skills (armed providers)
b. Massive/Exsanguinating Hemorrhage: Emphasis has shifted on the early recognition and control of severe bleeding in the tactical environment, mainly through use of extremity tourniquets, pressure dressings, hemostatic agents, and in other wounds, injectable hemostatic wound dressings or junctional tourniquets.
c. Airway: Depending on the environment, airway management may be as simple as basic adjuncts, such as head tilt chin lift, positioning, or nasopharyngeal airways which are ideal in causalities who maintain a gag reflex. Endotracheal intubation remains the gold standard for securing the airway, but this skill is seldom performed in the hot or warm zone due to equipment and time constraints. For deeply unconscious casualties without an airway, supraglottic devices can be quickly placed, or consideration made for emergent cricothyrotomy.
d. Breathing: The primary focus of breathing assessment is recognition and relief of tension pneumothorax. Penetrating wounds with high clinical concern can be treated with an occlusive chest seal. As highlighted in the ATLS 10th edition update9, needle thoracostomy should be performed at the lateral approach (4th/5th intercostal space, mid-axillary line) as this has higher initial success; it should be noted that providers should be familiar with team-specific equipment, to allow rapid access to the chest when needed (see Figure 3 below).
e. Circulation: Recognition and management of shock in trauma patients is key, however specific intervention in the hot zone is often limited. Depending on the distance to definitive care, interventions such as IV/IO access can be performed, combined with resuscitation using fluids, adjunctive agents like TXA, or even blood products should there be a delay to definitive care and transfusion is possible.
f. Disability: Assessment for traumatic brain injury with an AVPU scale, pupillary exam, as well as evaluate for gross neurologic deficit/possible spinal injury.
g. Exposure/Environment/Extremities/Everyone Else: Protect the casualty from hypothermia when feasible, and perform a full exposure to avoid missing additional injuries. If there are gross extremity injuries/deformities, splint them as able to prevent further injury and allow movement. It is also encouraged to have other team members self-check for injuries.
h. Fur?: Law enforcement K9s are ubiquitous around the U.S., and frequently integrated into tactical operations. Although K9 handlers are trained in first-aid measures, medical providers should have some familiarity with these procedures and equipment to further assist, particularly if a K9 handler is unable to provide care. It is important to note that some states, including Rhode Island, prohibit care of animals during routine EMS care, and providers should familiarize themselves with applicable state laws and regulations.

Figure 3: Needle decompression with a standard armor plate carrier in the anterior approach can be challenging (left), and accessibility may be greater with the lateral approach (right), consistent with updated ATLS guidelines. Providers should be familiar with armor used by operators to allow for assessment in place, or quick removal.

Figure 4: A sample plate carrier mounted load-out pouch for a TEMS provider, containing critical elements like tourniquets, chest seals, hemostatic gauze, and thoracostomy needles.
6. Secondary Assessment/Definitive Care: Remember that care continues after completion of the primary survey. When in the cold zone, a full secondary trauma survey should be performed, with vital signs, and all interventions as appropriate per standard trauma care guidelines. TEMS providers can be critical advocates for injured law enforcement officers when reaching definitive care, even if primary medical care is transitioned to an arriving EMS agency or receiving hospital.
SUMMARY
Tactical officers continue to play a critical role in responding to unique threats to law enforcement and the general public, a job that requires specialized medical care and support. TEMS remains a growing element of these operations, maintaining health/safety of law enforcement, and treating ill and injured patients/subjects encountered during operations. Although some areas of TEMS care carry controversial elements and continue to evolve, medical providers willing to support these operators contribute to the welfare and longevity of these critical assets in upholding public safety.
Additional Resources:
CONTOMS Course Offerings: Medical Director’s Course and EMT-T Course https://contoms.chepinc.org
Tactical Combat Casualty Care (TCCC) and Tactical Emergency Casualty Care (TECC): https://www.naemt.org
ACEP Tactical Medical Section: https://www.acep.org/how-we-serve/sections/tactical-emergency-medicine/
NAEMSP Operational EMS Committee: https://naemsp.org/membership/committees/operational-ems-fireground-hazmat-tactical/
Special Operations Medical Association (SOMA): http://www.specialoperationsmedicine.org/Pages/default.aspx
Johns Hopkins Tactical Medical Fellowship: https://www.hopkinsmedicine.org/emergencymedicine/fellowship_programs/tactical_medicine.html
AUTHOR: Matt LoConte, MD is a recent graduate of Brown University Emergency Medicine Residency at Brown University/Rhode Island Hospital.
Faculty reviewer: Heather Rybasack-Smith, MD is an EMS trained attending physician at Rhode Island Hospital.
REFERENCES
“Roman Medicine”, accessed at: https://www.unrv.com/medicine.php
“Genesis of the US Navy SEa Air and Land (SEAL) Teams”, accessed at: https://web.archive.org/web/20140222183844/https://navysealmuseum.com/about-navy-seals/seal-history-the-naval-special-warfare-story/genesis-of-the-u-s-navys-sea-air-land-seal-teams/
National Tactical Officer’s Association, TEMS Position Statement Affirmation, accessed at: https://www.ntoa.org/sections/tems/tems-position-statement/
Smith, ER, et al; “Incidence and Cause of Potentially Preventable Death after Civilian Public Mass Shooting in the US”, Journal of the American College of Surgery, Volume 229 Issue 3, September 2019
Counter Narcotics and Terrorism Operational Medical Support (CONTOMS): Medical Director’s Course Guidebook, provided for ACEP Medical Directors Course, October 2020
Counter Narcotics and Terrorism Operational Medical Support (CONTOMS): Tactical Medic Handbook, 2013 edition, accessed at: https://contoms.chepinc.org/sites/default/files/CONTOMS%20MEDIC%20HANDBOOK.pdf
Jamali, A; “Sick Call in TEMS”, presented at SOMA National Conference, May 16th, 2018, with supporting handout accessed at: http://www.specialoperationsmedicine.org/Documents/2018%20SOMSA/Handouts/TEMS_Sick_Call_Medicine.pdf
Updated TCCC Guidelines and Equipment Recommendations, accessed at: https://deployedmedicine.com
ATLS 10th Edition Highlights, accessed at: https://bulletin.facs.org/2018/06/atls-10th-edition-offers-new-insights-into-managing-trauma-patients/
Proposed EMS Bill for Rhode Island K9s, story featured on EMS1.com, accessed at: https://www.ems1.com/k-9/articles/ri-bill-seeks-ems-care-ambulance-transport-for-police-k-9s-1dFWoV4uqqmjposW/