Using POCUS for Ejection Fraction Estimation
Case:
A 73-year-old man presented to the emergency department (ED) for shortness of breath and orthopnea that had been worsening for the past 4-5 weeks. He has a past medical history of light chain amyloidosis, hypertension, hyperlipidemia, and diabetes.
His vital signs were significant for a heart rate of 110 beats per minute, blood pressure of 147/89, oxygen saturation of 97%, and he was breathing at 20 times per minute. Upon exam, he was in no acute distress, but did demonstrate mild orthopnea. He had pitting edema in his legs bilaterally, and had mild chest wall pain. An EKG, bloodwork, and chest X-ray were obtained. Point-of-care-ultrasound (POCUS) echo was performed to assess cardiac function.
The differential diagnosis included acute coronary syndrome, CHF exacerbation, pneumonia, and cardiac amyloidosis.
EKG showed sinus tachycardia with low voltage. Laboratory evaluation was unremarkable, with a negative troponin and high normal BNP. Chest radiograph showed bilateral infiltrates concerning for mild pulmonary congestion.
POCUS was obtained.
Figure 1: Parasternal Short View
Figure 2: Parasternal Long View
Figure 3: Apical 4-chamber View
Diagnosis:
Cardiac Amyloidosis.
Bedside echocardiography showed marked left ventricular hypertrophy with decreased ejection fraction. The parasternal long and short views show a markedly enlarged left ventricle, as well as the intraventricular septum. Qualitative assessment of left ventricle function elucidated a likely cause of heart failure for his presenting symptoms.
Discussion:
Ejection Fraction Assessment with POCUS Echocardiography
There are a multitude of ways to assess the cardiac contractility, as a surrogate for the left ventricular ejection fraction (LVEF), with POCUS. There are both qualitative and quantitative ways to go about this.
E-Point Septal Separation (EPSS) has been used since the 1970’s as a way to estimate LVEF in the setting of congestive heart failure and to risk-stratify patients. (1) EPSS is obtained in the parasternal long axis view and is a measure of the distance between the anterior mitral leaflet and the interventricular septum at its smallest distance, which occurs during diastole.
Measuring the EPSS:
In the parasternal long (PSL) view, align the M-mode marker with the anterior leaflet of the mitral valve at the location where it is closest to the interventricular septum.
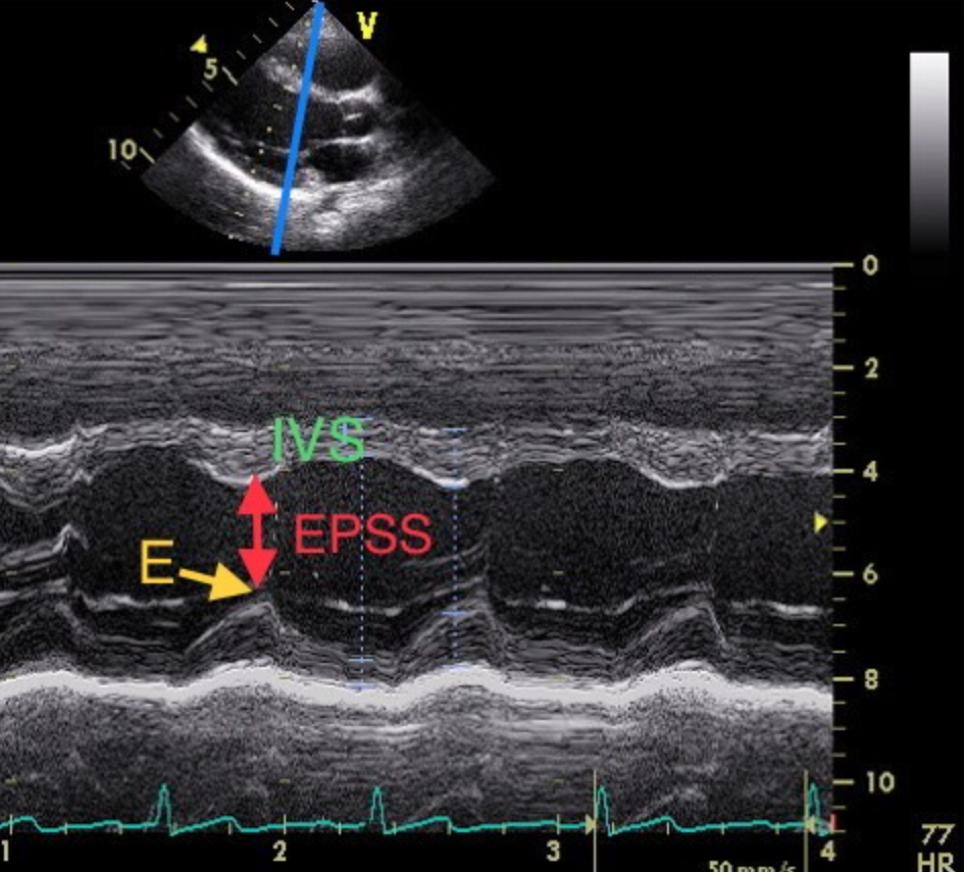
Figure 4: PSL view with motion mode to show EPSS (Cisewski, 2018)
The image should appear as “clouds over a mountain.” The EPSS measurement can be used as a continuous or discrete measurement. The generally accepted value of 7mm is used a cutoff, and an EPSS of greater than 7mm correlates with a LVEF of <50%.
Alternately, the EPSS can be used as a continuous measure in the formula:

EPSS is measured in mm, the other variables are constants.
EPSS can be impacted by aortic regurgitation and mitral stenosis, as such the measurements must be taken in the correct clinical context.
Fractional Shortening:
Another option for assessment of the LVEF is fractional shortening (FS).

FS should be evaluated in the parasternal long or parasternal short axis views. The FS is reported as a percentage, however, it is not equivalent to the LVEF. The normal range for FS is 30-45%, with larger percentages correlating with hyperdynamic left ventricles and lower percentages correlating with decreased LVEF. [1]
Measuring the FS:
In the parasternal long axis view, use M-mode across the left ventricle to measure the end diastolic left ventricular diameter, A---A in the image below, as well as the end systolic left ventricular diameter, B---B. The measurements can be used in the formula above to calculate the FS.

Figure 5: Apical 4-chamber view with motion mode to elucidate FS(Butts, 2014)
Similarly, this can be done in the parasternal short axis view:

Figure 6: Parasternal Short View with Motion mode to show FS(Gaspar, 2015)
Where EDD is the end diastolic diameter, and ESD is the end systolic diameter.
Most commonly, providers estimate LV function qualitatively at the bedside. When qualitatively assessing the LVEF the cardiac output is reported as hyperdynamic of normal (LVEF greater than 50%), moderate dysfunction (LVEF 30%-50%), and severe dysfunction (LVEF less than 30 In one meta-analysis, the qualitative estimation of LVEF had a sensitivity of 80.6% [5]. Qualitative assessment is done by looking at left ventricular contraction in at least 2 views. In the PSS view, you want to evaluate LV function at the level of the papillary muscles.
Both EPSS and FS can be utilized, in tandem or alone, to aid the provider in estimation of LVEF, as well as risk-stratify patients for disposition.
Case Resolution:
The patient was admitted to the medical service with a diagnosis of cardiac amyloidosis, leading to systolic heart failure. He was given multiple doses of furosemide for symptomatic management. He was placed on a salt-restricted diet and was seen by cardiology and hematology. He was eventually discharged on furosemide, spironolactone and the beginning course of a chemotherapeutic agent targeting light chain amyloidosis.
The POCUS assessment of this patient, with cardiac amyloidosis, is a perfect example of the utility of the EPSS and FS measurements to assess cardiac function and base clinical decisions.
Take-Aways:
POCUS Echocardiography is a quick and reliable way to assess LVEF
EPSS and FS can be quantitatively measured or qualitatively estimated
Valvular pathology can make EPSS difficult to ascertain reliably
Myocardial dysfunction, such as old ischemic events, can cloud estimation of FS
AUTHOR: Sean Bilodeau, DO is a PGY-1 in Emergency Medicine at the Warren Alpert Medical School of Brown University
FACULTY REVIEWER: Kristin Dwyer, MD is Ultrasound Faculty at Emergency Medicine at the Warren Alpert Medical School of Brown University
References:
Wong, M., Dr. (n.d.). Point-of-Care Echocardiography: A primer (Vol. 1). Ottowa: EMOttowa.
Cisewski, D., MD, & Alerhand, S., MD. (n.d.). Fellow corner: E-point septal separation in the patient with congestive heart failure. Retrieved March 31, 2021, from https://www.acep.org/how-we-serve/sections/emergency-ultrasound/news/dece/fellow-corner-e-point-septal-separation-in-the-patient-with-congestive-heart-failure/
Cisewski, D., MD, & Alerhand, S., MD. (2018, March 27). US probe: E-POINT Septal Separation (epss) in the Chf Patient (1283268951 946462936 M. Singh MD, Ed.). Retrieved March 31, 2021, from http://www.emdocs.net/us-probe-e-point-septal-separation-epss-in-the-chf-patient/
Butts, C. (2014). The speed of sound. Emergency Medicine News, 36(1), 9. doi:10.1097/01.eem.0000441173.81382.b2
Gaspar, H. A., & Morhy, S. S. (2015). The role of focused echocardiography in pediatric intensive care: A critical appraisal. BioMed Research International, 2015, 1-7. doi:10.1155/2015/596451
Martindale, J. L., Wakai, A., Collins, S. P., Levy, P. D., Diercks, D., Hiestand, B. C., . . . Sinert, R. (2016). Diagnosing acute heart failure in the Emergency Department: A systematic review and meta-analysis. Academic Emergency Medicine, 23(3), 223-242. doi:10.1111/acem.12878
Moore, C. L. (2002). Determination of left ventricular function by emergency physician echocardiography of hypotensive patients. Academic Emergency Medicine, 9(3), 186-193. doi:10.1197/aemj.9.3.186
Quarta, C. C., Kruger, J. L., & Falk, R. H. (2012). Cardiac amyloidosis. Circulation, 126(12). doi:10.1161/circulationaha.111.069195
Rapid estimation of left ventricular ejection fraction with ultrasound. (2018, November 15). Retrieved March 31, 2021, from http://aaemrsa.blogspot.com/2018/11/rapid-estimation-of-left-ventricular.html
Siadecki, S., MD, Saul, T., MD, & Lewiss, R., MD. (2015, February 03). Bedside ultrasound assessment of left VENTRICULAR function (1283274350 946466372 R. Solomon MD, Ed.). Retrieved March 31, 2021, from https://www.acepnow.com/article/bedside-ultrasound-assessment-left-ventricular-function/5/?singlepage=1
Vermeulen, M., & Levin, J. (2017, November 30). Management of shock: Bedside assessment of cardiac output. Retrieved March 28, 2021, from https://www.emra.org/emresident/article/management-of-shock-bedside-assessment-of-cardiac-output/