Age Matters: Managing Femur Fractures in Kids
In one overnight shift on the orthopedics service, our team evaluated three different pediatric patients with the same underlying injury: a femoral fracture. But, the management of all three children was different and the underlying reason for the different management was age.
Background:
Femoral shaft fractures are often seen in the pediatric population and are the most common cause of orthopedic hospitalizations in children (1). It is important to consider that the pediatric femur, in contrast to the adult femur, has a high capacity for remodeling and can tolerate more angulation, shortening, and rotational deformity than an adult femur (2).
Femoral fractures account for around 2% of all pediatric fractures and about 70% involve the shaft. There is a bimodal distribution affecting toddlers ages 2-4 and adolescents: additionally males are more commonly affected than females (2.5:1). In general, femur fractures occurring under the age of 10 are most commonly caused by a fall, whereas a motor vehicle collision is the most common etiology for ages greater than 10. (1, 2)
Diagnosis typically occurs with anterior/posterior and lateral x-rays of the femur. This allows for evaluation of not only the fracture location, but also the amount of displacement and configuration.

Figure 1. Citation: https://coreem.net/core/pediatric-femur-fractures/
management:
In our first case a four-month-old patient sustained a short oblique middle third diaphyseal femur fracture. Treatment: a Pavlik harness and close orthopedic follow up.
A Pavlik harness, shown below in figure 2, is a soft splint keeping the child’s legs in a neutral position, and is also used for hip dysplasia syndromes. Notably, the management for femur fracture is a Pavlik harness for any child less than six months old, regardless of the fracture pattern. There are no significant relative or absolute contraindications to a Pavlik harness.
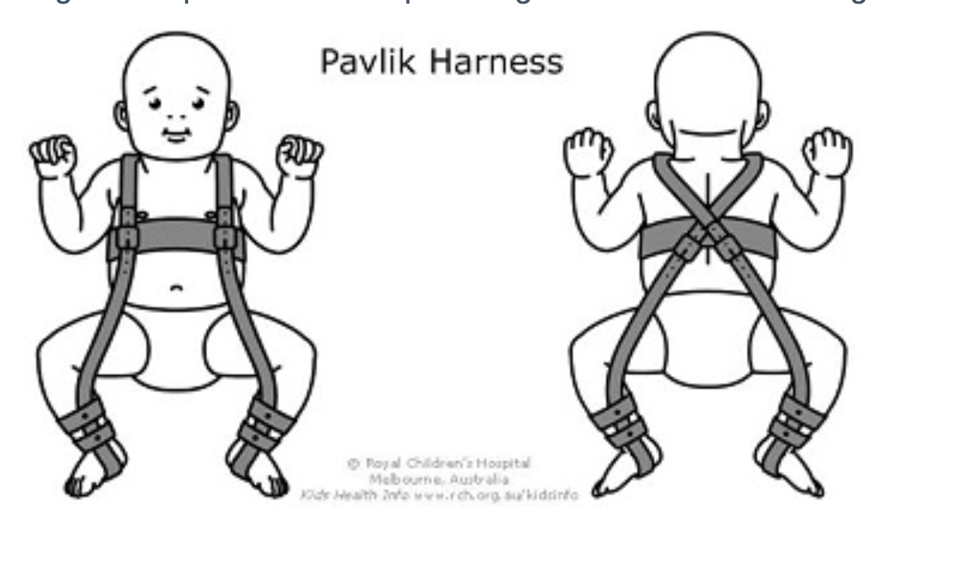
Figure 2. Citation: https://www.rch.org.au/kidsinfo/fact_sheets/Pavlik_Harness_for_DDH/
Our second case is a two-year-old male with a left spiral diaphyseal femur fracture. For this patient with a non-displaced, stable fracture our management included spica casting (shown below in Figure 3). In general, the management is spica casting for children between 6 months and 5 years old; however, relative contraindications include polytrauma, open fractures, and fractures that have more than 2 cm of shortening, any of which may require traction, delayed casting or operative fixation.

Figure 3. Citation: https://orthoinfo.aaos.org/globalassets/figures/a00424f03.jpg
For our third case, a nine-year-old sustained a proximal diaphyseal femur fracture and required operative management. Patients older than 5 will need operative management whether for intermedullary nail, internal fixation, or external fixation. Our patient went to the operating room to get flexible intramedullary nails on day two of admission to the hospital.
{kind=link}
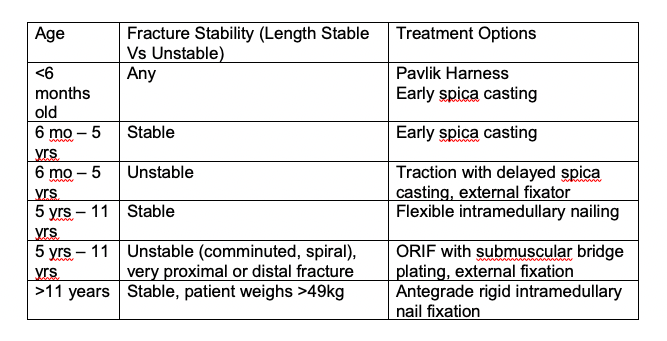
Table 1: Treatment options based on age and stability of femoral fracture (1-5)
Complications:
Several important complications to consider are: leg length discrepancy, malunion, and much more rarely nonunion, but all femur fractures will require ongoing orthopedic follow up regardless of initial management.
Non-Accidental Trauma:
A word on non-accidental injury: no individual fracture type can distinguish an accidental from a non-accidental injury. When a pediatric patient presents with a femur fracture, regardless of age, non-accidental trauma should be highly suspected. One potential predictor of whether or not a pediatric femoral fracture is caused by non-accidental injury is whether or not the child knows how to walk (6). In children who are too young to walk, up to 80% of femoral fractures have been attributed to abuse. But, even in a child who is walking, there should be a suspicion of NAT. As always, it is vital to take a good history and investigate the mechanism of the fracture.
Take-Aways:
Age plays a pivotal role in pediatric femur fractures
Patients who are younger than 5 may not need surgery
Older and heavier children follow similar rules as adults
As always maintain a high degree of suspicion for NAT
Author: Anita Knopov, MD
Faculty Reviewer: Meghan Beucher, MD
References:
Edgington J, Shirley E, Sink. “Femoral Shaft Fractures.” Orthobullets. Orthobullets.com. Web. 5/6/2020.
Sela Y, Hershkovich O et al. Pediatric femoral shaft fractures: treatment strategies according to age - 13 years of experience in one medical center. J Orthop Surg Res. 2013; 8:23.
Aylyarov Ilya MD. Pediatric Femur Fractures. 12 Sept. 2018, https://coreem.net/core/pediatric-femur-fractures/ Accessed March 25, 2021/
Felluga, Dino. Guide to Literary and Critical Theory. Purdue U, 28 Nov. 2003, www.cla.purdue.edu/english/theory/. Accessed 10 May 2006.
May C; Hedequist D. Femur Fracture. Pediatric Orthopedic Society of North America. https://posna.org/Physician-Education/Study-Guide/Femur-Fracture. Accessed March 25, 2021.
Schwend RM, Werth C, Johnston A. Femur shaft fractures in toddlers and young children: rarely from child abuse. J Pediatr Orthop. 2000 Jul-Aug; 20(4):475-81.