Evaluation And Care Of Pediatric Patients After Sexual Assault
CASE
A 15-year-old female presents to your emergency department with her mother. She is tearful and withdrawn. She tells you that she was sexually assaulted by a 20 year old male acquaintance 2 days prior. She reports that she would like to report the assault and would like to have a forensic exam. She is having some vaginal bleeding and pain around her rectum. She admits to using alcohol and some marijuana on the night of the assault. She is unable to remember everything that happened and thinks her assailant may have put a drug in her drink.
DISCUSSION
Background
“Sexual assault” is a comprehensive term that includes any forced or inappropriate sexual activity. [1] Unfortunately, this is not an uncommon chief complaint we encounter in the ED. The 2015 National Intimate Partner and Sex Violence (NIPV) Survey found that 43.6% of US women and 24.8% of US men experienced some form of contact sexual violence in their lifetime and 21.3% of US women and 2.6% of US men reported attempted or completed rape. [2] Adolescents represent a majority of sexual assault victims, with a peak incidence at 16 to 19 years old. [3] Eight-one percent of females and 70.8% of males reported the first rape they experienced occurred when they were less than 25 years old.
Adolescents are more likely to be assaulted by an acquaintance or relative and also to delay medical evaluation. Younger children are more likely to be assaulted by a member of their extended family and they have even greater barriers to report their abuse because they are often dependent on their abuser who may have the ability to manipulate and/or silence the child. Because of this, the abuse may be ongoing for weeks, months, or years before it is reported. In a study by Jones, JS in 2003, 39% of adolescent victims in their cohort had a history of previous sexual abuse. [4] Other data has shown that adolescents with a history of abuse may have feelings of powerlessness to stop sexual assault, have difficulty with boundary setting, or have confusion about normal dating and sexual relationships leading to higher risk of additional sexual assaults. [4]
Where to start
As with any other patient, it is important to assess for and manage any medical emergencies, starting with the ABCs. Adolescent patients are more likely to experience ano-genital injuries and less non-genital injuries compared with adult survivors of sexual assault. [4] However, you should still consider possible associated blunt or penetrating trauma. [5] Once the acute medical concerns have been addressed, move the patient to a quieter and more private location to discuss what happened. It can also be beneficial to discuss with patients and their families what to expect and that the whole process can take several hours.
When taking a history, it is important to remember to use developmentally appropriate language, remain committed to addressing the needs of the patient during the exam, giving them the power to make choices whenever possible, and supporting their healing and growth while avoiding retraumatization. [6] In younger children especially, “minimal interview” techniques should be used to prevent distortion of the disclosure or inconsistent histories. [7] With children and adolescents, it’s also important to recognize that parents or caregivers may also need strategies to support their child and help coping with their own distress. [8] The process of evaluation after an assault should not only asses your patient’s health concerns, it should also provide emotional support for the patient and their caregivers, and coordinate medical, psychological, and legal resources. [6]
It can be very difficult to make time to do a thorough and uninterrupted exam during a busy ED shift, but the way these cases are handled can have a lasting effect on how your patient processes the trauma. Up to 1/3 of sexual assault survivors have PTSD and they are 13 times more likely to attempt suicide. Providing accurate information and responding in a supportive manner to patients’ disclosure of feelings of blame or shame about the event, as well as fears of permanent physical or emotional damage can mediate development of trauma symptoms. [9,10]
Mandated Reporting
Physicians are required to report all cases of sexual assault of a minor to law enforcement and an allegation or concern for abuse is enough to trigger a report. [11] If there is concern that there are other children who may have had contact with the abuser (i.e. siblings of the abused child), this must also be reported. [8] These other affected children will also need a medical screening exam, but this does not necessarily need to happen in the ED; it can often be done at their pediatrician’s office. Although we are required to report known or suspected abuse, it does not mean our patients must speak with the police.
The Forensic Exam
If the stress of these patient interactions isn’t enough, there is the added complication of collecting data with the forensic exam. First, it’s important to know who to offer the exam to and when. Laws vary by state, but usually the timeline to collect evidence is 72 hours to 5 days after the assault. It is important to inform your patient that the point of the forensics exam is to collect evidence, but it does not mean they are required to report the assault. Even if the patient is undecided about reporting, it is important to discuss the option of the forensics exam so that if they decide to report later they will have physical evidence to use in court. [12]
Patients must be able to provide consent for the forensic exam and they have the right to refuse any or all parts of the exam once it has begun. If a patient is intoxicated, they should be given time to sober before they can consent to the exam. Minors who cannot legally give consent but are old enough to assent to the exam also have the right to decline the exam, even if their parent or guardian insists on it. [12]
If possible, try to provide an advocate to assist the patient during the exam and provide more information on legal options. In Rhode Island, Day One is the program we use. Advocates provide information and support to patients through the process of the exam and as well as help them with making statements to the police. [13] Calling them early can help with timing.
The goal of the exam is to provide care that respects the emotional and physical needs of the victim while collecting the best possible forensic evidence. It can be performed at any hospital by any licensed provider, but, especially in children and adolescents, it is preferable that the exam be done by a SANE or child-abuse trained physician or mid-level provider if they are available. The exam itself requires asking invasive questions, collecting the patient’s clothes (including underwear) if they were worn during the assault, swabs of the mouth, genitals, and skin, and pictures of any injuries. It can be a stressful experience for both the provider and the patient and the provider should be familiar with the elements of the exam to help it go as smoothly as possible. The provider must remain in the room until the exam is complete to maintain the evidence chain of command, so some planning beforehand is important before you disappear from your shift for an hour.
The details of the forensics exam are beyond the scope of this post, but this website is an excellent resource: https://www.safeta.org/page/examresources. It is important to familiarize yourself with the components of the exam and plan ahead with supplies you will need. Below are images of a kit used in RI. This link (https://www.youtube.com/watch?v=vRcR8s6oQtg&ab_channel=ACASAArkansas) provides a step-by-step guide to the exam.

Figure 1: Elements to include in documentation for the forensics exam.

Figure 2: Components of the SANE kit
Workup
Medical work-up for these patients is based on your exam and physical. If there is concern for drug-facilitated assault, blood and urine samples should be collected to test for drugs and alcohol. Unfortunately many substances used in sexual assaults (ex. Rohypnol, GHB, and ketamine) are often not seen on UDS because of their short half-life or the metabolites are just not on the UDS panel. [14]
The decision to test for STI’s in children/adolescents should be made on a case by case basis. However, if there are any high risk features, testing should be more strongly considered. These features include: signs/symptoms of genital discharge, itching, lesions, or ulcers, or evidence of genital or oral penetration or ejaculation, suspicion that the assailant has or is at high risk of having an STI, the patient’s family member has an STI, or the patient or parent requests testing. [7] If you are seeing the patient shortly after the assault, these tests are often just a baseline as they would not reflect a transmitted STI yet. These patients should be counseled on the possible need for repeat testing in a few weeks. This can be done as an outpatient.
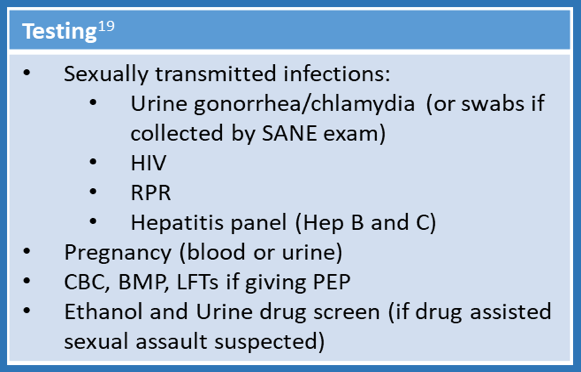
Figure 1: List of recommended tests in evaluation of sexual assault in the ED
Treatment
All patients who have been sexually assaulted should be offered STI prophylaxis for gonorrhea, chlamydia and trichomonas. [15,16] Testing for syphilis should be offered if prevalence is high in your area and treatment should be provided only if the test is positive. [7]
The decision to give post-exposure prophylaxis (PEP) for HIV should be made after a discussion with the patient. PEP is indicated if there was genital, oral, or anal contact with the assailant’s genitals semen, or blood. It should not be given if the assault occurred >72 hours prior. The risk of HIV transmission from a single sexual assault is less than 0.1% and PEP does have side effects (diarrhea, nausea, headache, fatigue, and stomach pain are most common), so this is an important conversation to have with your patient and should involve discussion of assailant and victim risk factors. [17] If the patient does choose to take it, they must begin it within 72 hours of the assault, they must adhere to dosing, and they should have close follow up. [15] You can provide your patient with a one-week supply of medication and schedule follow up within 1 week to discuss side effects and tolerance. Repeat HIV testing should be done for all sexual assault victims at 6 weeks, 3 months, and 6 months after the assault.
Unimmunized patients should also be offered the hepatitis B vaccine, which will require a 2nd dose at 1-2 months and a 3rd dose at 4-6 months. If the patient is unvaccinated and the assailant is known to have HBV, you can also consider giving hepatitis B immunoglobulin. [7] Females 9- 26 years old and males 9-21 years old should be offered the HPV vaccine if they have not had it. [15]
The risk of pregnancy after an assault is approximately 5%; a pregnancy test should be obtained and emergency contraception (EC) should be offered to any female of reproductive age. [7] EC is most effective when taken as soon as possible after the assault, but can be given up to 5 days after the assault. Patients who take it must also be instructed to follow up with care if their menstrual cycle is delayed more than 1-2 weeks since it can fail. Anti-emetics should also be given along with the emergency contraceptives since vomiting is a common side effect. [7]

Figure 2: Recommended prophylactic treatment for STIs, HIV, and emergency contraceptives for victims of sexual assault.
TAKE-AWAYS
Sexual assault is not uncommon and adolescents represent the majority of victims.
Suspected or confirmed sexual assault of a minor must be reported to law enforcement.
Make sure to do a thorough medical evaluation and stabilization of your patient before the forensic exam.
The forensics exam should be offered to all eligible patients, but having the exam does not mean they have to report the assault to police.
Be familiar with the steps of the exam and pay attention to your patient’s psychological well-being throughout the assessment.
Test for and offer STI prophylaxis and emergency contraception, discuss risk factors with patient before prescribing HIV PEP.
AUTHOR: Hannah Chason, MD is a third year emergency medicine resident at Brown University/Rhode Island Hospital.
FACULTY REVIEWER: Meghan Beucher, MD is a pediatric emergency medicine attending at Hasbro Children’s Emergency Department.
REFERENCES
1. Kaufman M. Care of the Adolescent Sexual Assault Victim. Pediatrics. 2008;122:462-470. doi:10.1542/peds.2008-1581
2. CDC. National Intimate Partner and Sexual Violence Survey: 2015 Data Brief-Update Release. Atlanta, GA Natl Cent Inj Prev. 2015:1-124. https://www.cdc.gov/violenceprevention/pdf/2015data-brief508.pdf.
3. Poirier MP. Care of the female adolescent rape victim. Pediatr Emerg Care. 2002;18(1):53-59. doi:10.1097/00006565-200202000-00016
4. Jones JS, Rossman L, Wynn BN, Dunnuck C, Schwartz N. Comparative Analysis of Adult versus Adolescent Sexual Assault: Epidemiology and Patterns of Anogenital Injury. Acad Emerg Med. 2003;10(8):872-877. doi:10.1197/AEMJ.10.8.872
5. emDOCs.net – Emergency Medicine EducationManaging Sexual Assault in the Emergency Department - emDOCs.net - Emergency Medicine Education.
6. Edition S. A National Protocol for Sexual Assault Medical Forensic Examinations - Adults/Adolescents First Edition.; 2004.
7. Riviello RJ, Rozzi H V. Evaluation and Management of the Sexually Assaulted or Sexually Abused Patient Second edition. 2013:1-177.
8. Department of Justice U, on Violence Against Women O. April 2016 A National Protocol for Sexual Abuse Medical Forensic Examinations Pediatric.; 2016.
9. Danielson CK, Holmes MM. Adolescent sexual assault: An update of the literature. Curr Opin Obstet Gynecol. 2004;16(5):383-388. doi:10.1097/00001703-200410000-00005
10. Adams JA, Kellogg ND, Farst KJ, et al. Updated Guidelines for the Medical Assessment and Care of Children Who May Have Been Sexually Abused. J Pediatr Adolesc Gynecol. 2016;29(2):81-87. doi:10.1016/j.jpag.2015.01.007
11. Dos and Don’ts for Pelvic or Genitourinary Exams in Minors - ACEP Now.
12. Know the Legal Requirements When Caring for Sexual Assault Victims - ACEP Now.
13. Advocacy | Day One.
14. Dinis-Oliveira RJ, Magalhães T. Forensic toxicology in drug-facilitated sexual assault. Toxicol Mech Methods. 2013;23(7):471-478. doi:10.3109/15376516.2013.796034
15. CDC. Sexual Assault and Abuse and STDs - 2015 STD Treatment Guidelines.; 2015. http://www.cdc.gov/std/tg2015/sexual-assault.htm. Accessed September 6, 2015.
16. St. Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s Treatment Guidelines for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(50):1911-1916. doi:10.15585/mmwr.mm6950a6
17. Hoehn EF, Overmann KM, Fananapazir N, et al. Improving Emergency Department Care for Pediatric Victims of Sexual Abuse.
18. CDC. Updated Guidelines for Antiretroviral Postexposure Prophylaxis After Sexual, Injection-Drug Use, or Other Nonoccupational Exposure to HIV—United States, 2016.; 2016.