Just One Bite: An Unusual Case of Abdominal Pain
CASE
A 64-year-old male with a history of hypertension, glaucoma, and central retinal vein occlusion presents to the emergency department in August with 2 weeks of progressively worsening, non-radiating abdominal pain. He describes feeling something “stuck” in his upper abdomen. He developed a dry cough around the same time as the abdominal pain and finds that coughing exacerbates the pain. He has tried milk of magnesia twice without relief. He has noticed a decreased appetite and a 7-pound weight loss. He also reports fatigue, chills, and myalgias.
He is a former smoker and a former daily drinker, now only drinking 5 beers on the weekends. He lives in Rhode Island, although he is originally from the Dominican Republic and last visited there 2 months ago. He works in exercise machine assembly and packing. He enjoys gardening.
Vital signs are normal. Physical exam reveals tenderness to palpation in the right upper quadrant, left upper quadrant, and epigastrium. There is also right and left costovertebral angle (CVA) tenderness.
Basic labs were notable for hemoglobin 11.4, platelets 116, sodium 131, creatinine 1.12, and normal LFTs and lipase. A chest x-ray and CT abdomen were obtained as shown below.
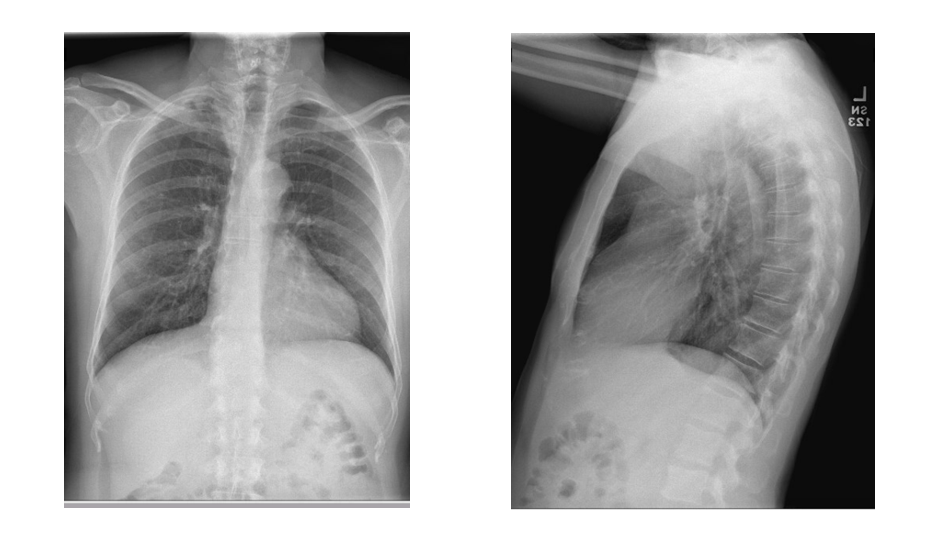
Image 1. Chest x-ray
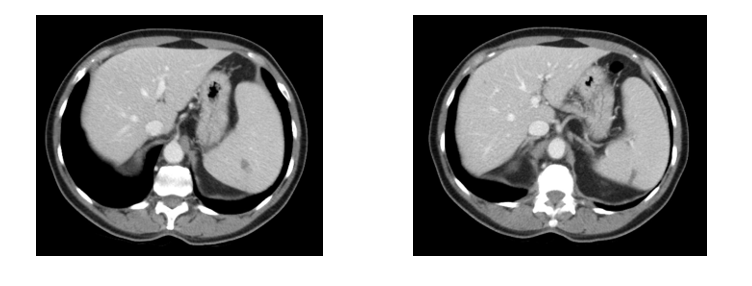
Image 2. CT imaging
A single test was ordered in the emergency department that confirms the diagnosis.
TEST AND DIAGNOSIS
A blood parasite smear showed scattered red blood cells with intraerythrocytic small ring form parasites and occasional red blood cells with 4 intraerythrocytic ring form parasites. Degree of parasitemia was 0.7%.
This confirmed the diagnosis of babesiosis.

Image 3. Red blood cells with intraerythrocytic small ring form parasites
DISCUSSION
Background
Babesiosis, also called “Nantucket fever” and “the malaria of the United States,” [1,2] is a protozoan infection caused by Babesia microti. Babesiosis is endemic in the Northeastern and upper Midwestern parts of the Unites States.
Babesiosis was first reported in cattle in 1888 by Victor Babeș. [3] The first case of human babesiosis was reported in 1957 in an asplenic patient. The first report of babesiosis in an immunocompetent patient was in 1969. [2,3]
The lifecycle of B. microti involves two hosts, typically the white-footed deer mouse and the Ixodes scapularis tick. When the tick bites the mouse, it introduces sporozoites into the bloodstream of the mouse. The sporozoites then enter the red blood cells, form ring-shaped trophozoites, and undergo asexual reproduction to form tetradic merozoites. The red blood cell lyses, releasing merozoites back into the bloodstream. Most will invade new red blood cells, but some will differentiate into gametes which are then ingested by the next tick to bite the mouse. Inside the tick, the gametes undergo fertilization and form sporozoites. [4,5]
Humans are not a necessary part of the life cycle of B. microti but enter the life cycle when bitten by an infected tick. Just as in the mouse, sporozoites will enter human red blood cells and undergo asexual reproduction. Humans are considered dead-end hosts as they do not typically transmit the disease to other organisms. [4] However, human-to-human transmission rarely occurs transplacentally and via contaminated blood transfusions. [1-6]
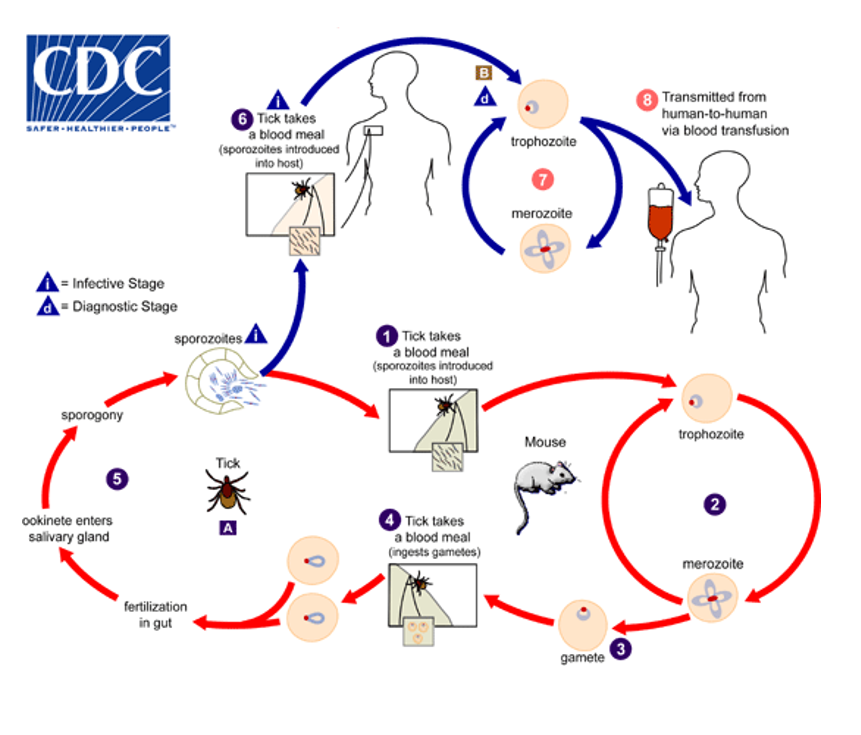
Figure 1. Life cycle of B. microti
B. microti is the most frequent transfusion-transmitted parasite, and since it resides in red blood cells, typical techniques like leukoreduction are not effective at reducing transmission. [3] There have been over 250 cases of transfusion-transmitted babesiosis since 1980. [6] In 2019 the FDA recommended regional blood donor screening for babesiosis, which has greatly reduced the risk of transfusion-transmitted babesiosis. [6,7]
Clinical Manifestations
The release of merozoites into the bloodstream causes hemolysis, which is the cause of the constitutional symptoms, anemia, and jaundice. [5] Since the spleen plays a major role in protecting against B. microti by clearing infected red blood cells from circulation, patients who are over age 50, asplenic, or otherwise immunocompromised are at risk for severe disease. Complications can include acute respiratory distress syndrome (ARDS), disseminated intravascular coagulation (DIC), congestive heart failure (CHF), renal failure, coma, and death. [2,3,5] The mortality of patients hospitalized with all forms of babesiosis is up to 10%, and is even higher among the immunocompromised. [1]
This patient had splenic infarction, which is a rare complication of babesiosis. Unlike the other complications of severe babesiosis, both splenic infarction and splenic rupture can occur in young, healthy patients. However, they still carry a significant mortality rate of 5.8%. [2] The first cases of babesiosis causing splenic infarction were published in 2007. [8] The pathophysiology is not entirely understood, but it is likely due to formation of microthrombi causing tissue necrosis or deformed infected red blood cells causing obstruction in the vasculature. [1-3,8]
Diagnosis
Babesiosis should be considered in patients who live in, or recently traveled to an endemic area, especially those over age 50 or immunocompromised who present with new organ failure. A history of a known tick bite can be helpful, but because the ticks are so small, bites are often unnoticed, and therefore, a lack of reported tick bite cannot rule out the disease.
Laboratory findings include signs of hemolytic anemia (low haptoglobin, elevated lactate dehydrogenase (LDH), hyperbilirubinemia), thrombocytopenia, and hyponatremia. Liver enzymes are often - but not always - elevated. [2,3,5]
The diagnosis is confirmed by peripheral blood smear. Trophozoites will appear as intraerythrocytic, round, ring-form parasites. However, they are not specific as they closely resemble those seen in the early stages of Plasmodium falciparum infection. In a patient who recently traveled to a malaria endemic area, it can be hard to distinguish these diseases based on this finding alone. The textbook “Maltese Cross,” which is the tetrad of merozoites undergoing asexual budding, is pathognomonic for babesiosis. [2,3,5]
Co-infection with the other diseases carried by the Ixodes tick, including Lyme, anaplasmosis, and Powassan virus is not uncommon. Empiric treatment with doxycycline is recommended while awaiting confirmatory testing. [4]
Treatment
The recommended treatment for mild to moderate disease is atovaquone plus azithromycin for at least 7 to 10 days. For severe disease, quinine plus clindamycin is recommended. Exchange transfusion is recommended in patients with parasitemia >10%, hemoglobin <10, or pulmonary, liver, or renal impairment. [5]
CASE RESOLUTION
The patient was admitted to the hospital and started on azithromycin, atovaquone, and empiric doxycycline. He was discharged 2 days later. At his 2 week follow-up appointment in clinic, his symptoms were resolved. His blood parasite smear at that time showed no residual parasitemia.
TAKE-AWAYS
· Symptoms can range from mild flu-like illness to severe, fulminant infection
· Consider babesiosis in elderly or immunocompromised patients with a flu-like illness during summer months in endemic regions
· Splenic infarction is a rare but potentially fatal complication that can be seen even in mild infection
· Early diagnosis and treatment prevent life-threatening complications
Author: Danielle Kerrigan, MD is a third-year resident at Brown University/Rhode Island Hospital
Faculty Reviewer: Melanie Lippmann, MD is an Associate Professor of Emergency Medicine at Brown University and an attending physician at Rhode Island Hospital and The Miriam Hospital
ReferenceS
1. Alvi, A., Gupta, S., Goyal, P., Pichardo, J., & Mattana, J. (2019). Splenic infarction as a rare presentation of severe babesiosis. Idcases, 15, e00491. doi: 10.1016/j.idcr.2019.e00491
2. Dumic, I., Madrid, C., Rueda Prada, L., Nordstrom, C., Taweesedt, P., & Ramanan, P. (2020). Splenic Complications of Babesia microtiInfection in Humans: A Systematic Review. Canadian Journal Of Infectious Diseases And Medical Microbiology, 2020, 1-8. doi: 10.1155/2020/6934149
3. Gupta, A., Patel, P., Manvar, K., Kellner, T., & Guevara, E. (2019). Splenic infarction in babesiosis: A rare presentation. Clinical Case Reports, 7(8), 1591-1595. doi: 10.1002/ccr3.2301
4. Centers for Disease Control and Prevention (CDC). (2022). Babesiosis. Retrieved 15 September 2022, from https://www.cdc.gov/parasites/babesiosis/
5. Vannier, E., Diuk-Wasser, M., Ben Mamoun, C., & Krause, P. (2015). Babesiosis. Infectious Disease Clinics Of North America, 29(2), 357-370. doi: 10.1016/j.idc.2015.02.008
6. Bloch, E., Krause, P., & Tonnetti, L. (2021). Preventing Transfusion-Transmitted Babesiosis. Pathogens, 10(9), 1176. doi: 10.3390/pathogens10091176
7. US Food and Drug Administration (FDA). (2022). Recommendations for Reducing the Risk of Transfusion-Transmitted Babes. Retrieved 15 September 2022, from https://www.fda.gov/regulatory-information/search-fda-guidance-documents/recommendations-reducing-risk-transfusion-transmitted-babesiosis0.3201/eid1808.110988
8. Florescu, D., Sordillo, P., Glyptis, A., Zlatanic, E., Smith, B., Polsky, B., & Sordillo, E. (2008). Splenic Infarction in Human Babesiosis: Two Cases and Discussion. Clinical Infectious Diseases, 46(1), e8-e11. doi: 10.1086/524081
9. Dumic, I., & Severnini, E. (2018). “Ticking Bomb”: The Impact of Climate Change on the Incidence of Lyme Disease. Canadian Journal Of Infectious Diseases And Medical Microbiology, 2018, 1-10. doi: 10.1155/2018/5719081
10. Joseph, J., Purtill, K., Wong, S., Munoz, J., Teal, A., & Madison-Antenucci, S. et al. (2012). Vertical Transmission of Babesia microti, United States. Emerging Infectious Diseases, 18(8).