Will Achilles Heal? When Calcaneal Fractures Are Surgical Emergencies

“Any fracture that threatens the skin integrity of the posterior heel is an orthopedic surgical emergency…”
CASE
A 20-year-old otherwise healthy male presents to the emergency department for right lower extremity pain after being tackled during a football scrimmage two days ago. He thought it would get better over time by taking ibuprofen, but still cannot walk on it. He has since experienced significant pain from his right heel extending upwards.
On physical exam, he is tachycardic, with a heart rate of 105. Vital signs are otherwise normal. He is in obvious discomfort, though not acute distress. He has tenderness and swelling of the right heel, with prominent ecchymosis posteriorly (fig. 1). There is no “gap” palpated at the Achilles tendon. However, the area superior to the posterior heel is firmly indurated. The right lower extremity is neurovascularly intact and range of motion is limited secondary to pain. He denies paresthesias or numbness. The examiner is unable to complete the Thompson test secondary to pain.
Note: The Thompson test serves to test the integrity of the Achilles-calcaneal axis. The examiner squeezes the patient’s calf and a positive result is elicited with absence of resulting plantarflexion. This would raise concern for disruption of the Achilles-calcaneal axis, e.g. Achilles tendon rupture or avulsion fracture.

Fig. 1: Representative Physical Exam Findings (Journal of Emergency Medicine [1]).
Given the above, the provider orders plain films of the right lower exremity and is surprised to discover the representative findings below:

Fig. 2: Radiograph representing our patient’s calcaneal fracture (AO Foundation [2]).

Fig. 3: Anatomic reorientation of normal calcaneal anatomy on lateral radiograph
(StatPearls; inlay title obscured [3]).
DIAGNOSIS
A “tongue-type” (or “beak-type”) calcaneus fracture is demonstrated above in figure 2, which involves the posterior calcaneal tuberosity (PCT). Note the subtle skin tenting of the posterior heel in figure 2, which might be easily overlooked on physical exam with an earlier (i.e. acute) presentation. Gardner, et al. 2008, reviewed outcomes of 29 patients with posterior skin compromise at presentation including 12 with threatened skin, 10 with partial thickness breakdown, and 7 with full thickness breakdown. They found that posterior skin compromise was less likely to be associated with a fall mechanism, and often roughly correlated with degree of fracture displacement. [4] While a CT scan is usually required at some point for these injuries and is important to determine degree of displacement and joint involvement, CT scan is usually best deferred to the receiving facility. Do not delay orthopedic consultation or patient transfer (if required) to obtain advanced imaging of the calcaneus.
DISCUSSION
Emergency physicians must be able to recognize which calcaneal fractures are surgical emergencies. As a general rule, any fracture that threatens the skin integrity of the posterior heel is an orthopedic surgical emergency. These include tongue-type or beak-type calcaneal fractures as well as avulsion fractures of the posterior calcaneal tuberosity (e.g. the intact Achilles can pull a piece of bone upwards). When the bone fragments exert pressure on the thin and poorly vascularized skin of the posterior heel, skin necrosis is often the outcome if not promptly surgically repaired within 6 hours [2]. If allowed to come to fruition, these injuries are frequently complicated by infections, chronic wounds, foot amputations and/or death. Skin graft/reconstruction in this area is exceedingly difficult due to the poor blood supply. Particularly poor outcomes can be expected in patients who smoke, have diabetes, have peripheral vascular disease, etc. [5]

Fig. 4: Skin necrosis of the posterior heel secondary to PCT fracture (AO Foundation [2]).
Fracture Morphologies
A “tongue-type” or “beak-type” fracture occurs when the calcaneus is fractured through the PCT horizontally. The strong insertion of the Achille’s upon the superior fracture fragment causes its cephalad displacement (then resembling an opened mouth) and exerts pressure on the posterior heel skin. “Tongue-type” and “beak-type” are—to the emergency physician—clinically synonymous terms stemming from the different classification systems; you will generally see and hear them used interchangeably. In “sleeve-type” fractures, cephalad-displaced avulsion fractures of the PCT can also lead to pressure necrosis [6]. All of these fractures can present with subtle physical exam and imaging findings. The Essex-Lopresti and Beavis/Lee classification systems exist to facilitate pattern recognition of these fractures and guide management
Essex-Lopresti Classification
In 1952, Essex-Lopresti attempted to broadly categorize calcaneus fractures into either depression-type (fig. 5) or tongue-type (fig. 6) fractures based upon lateral plain radiographs. In these fractures, a downward and significant axial load force (green arrows in figures below) causes the lateral process of the talus to act as a wedge to fracture the calcaneus. The two types share a common primary fracture line and differ based upon where the secondary fracture lines exist. As identified in this classification system, all tongue-type fractures (fig. 6) are surgical emergencies. [7]

Fig. 5: Depression-type fracture: notice the secondary fracture line typically exits vertically/superiorly just posterior to the posterior calcaneal facet (AO Foundation [2]). For brief review of anatomy, return to fig. 3.

Fig. 6: Tongue-type fracture: notice the secondary fracture line exits horizontally and thus splits the PCT into superior and inferior halves (AO Foundation [2]).
Tongue-type is always a surgical emergency.
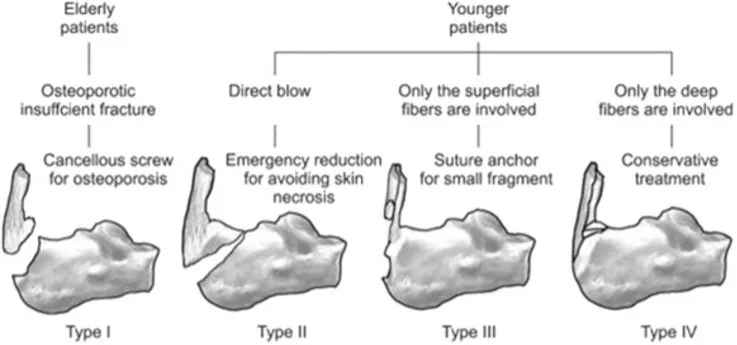
Fig. 7: Beavis/Lee classifications of posterior calcaneal tuberosity avulsion fractures.
Type II (“beak-type”) is always a surgical emergency. Types I (“sleeve-type”) and III are potential surgical emergencies that depend on degree of displacement and potential for skin compromise.
Interestingly, Carnero-Martin de Soto, et al. reviewed 21 patients with PCT fractures and found that Beavis type I vs type II did not change the incidence of post-surgical skin compromise and instead, found that the degree of displacement was more clinically significant. With less than or equal to 2 cm displacement, no patients had skin compromise, whereas if displacement was greater than 2 cm, 45% of patients had post-op soft tissue compromise (p=0.035). [9]
MANAGEMENT
After a calcaneal fracture is identified on lateral plain films, transfer to higher level of care should be considered early. Any type of calcaneal fracture that threatens the skin of the posterior heel is a surgical emergency. As specifically discussed, Beavis/Lee Types I & III fractures are surgical emergencies if sufficiently displaced. Beavis/Lee Type II “Beak-type” and Essex-Lopresti “Tongue-type” calcaneal fractures are always surgical emergencies even in absence of evidence of skin compromise. In addition to these fracture types, all intra-articular, displaced, or comminuted calcaneal fractures require immediate orthopedic consultation. A CT scan will often help to clarify management and eventual surgical planning though, importantly, should not delay orthopedic evaluation or a necessary transfer. While non or minimally-displaced extra-articular calcaneal fractures typically only require orthopedic outpatient follow-up, a Beavis/Lee Type I fracture pattern is an example of an extra-articular fracture that could be a surgical emergency depending on degree of displacement identified on CT scan.
Splinting
Until definitive management is available, all calcaneal fractures will benefit from immobilization, application of a posterior leg splint, elevation (keep in mind risk of compartment syndrome), non-weight bearing status, and analgesia. The goal of splinting this injury is to both immobilize and to minimize/remove pressure off of the posterior heel skin. The most common is the Bulky Jones Dressing/Splint, but we prefer a modified posterior leg splint, as seen below. This technique was described by by Hsu, et al. in 2013, also of Brown University, and is demonstrated below: [10]
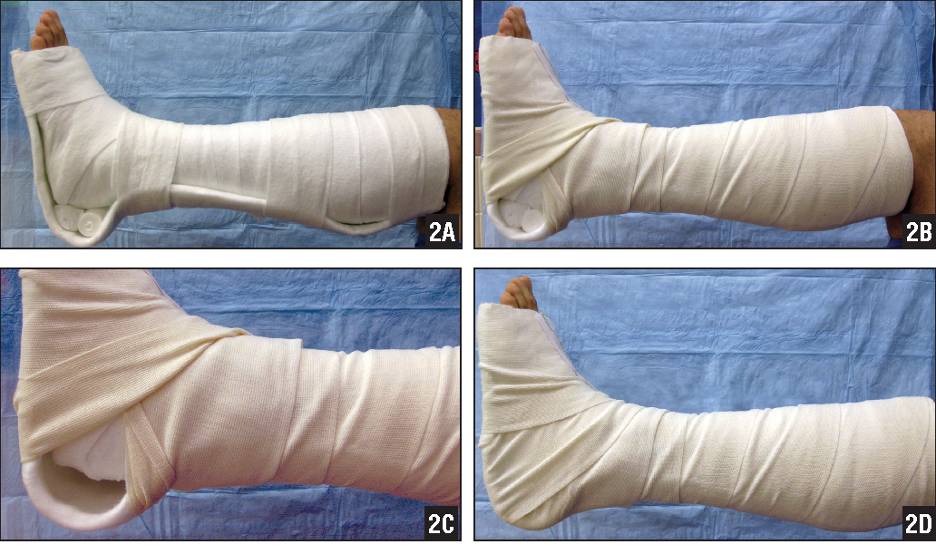
Fig. 8. Posterior leg splint technique to minimize posterior heel skin pressure/avoid heel ulcers. [10]
Create the splint as you would any posterior leg splint though with a few slight modifications: When forming the splint, insert two small rolls of Webril or bulky rolled gauze until the splint hardens. Then, remove these rolls when completing your splint by temporarily creating a window in the ACE wrap. The foot should be in 30 degrees of plantarflexion to relieve soft tissue tension on the skin of the posterior heel. In our opinion, choosing Ortho-Glass® will facilitate this technique over plaster.
TAKE AWAYS
Always examine the posterior heel looking for evidence of threatened skin (foot fractures are often initially missed in poly-traumas)
Any fracture that threatens the skin integrity of the posterior heel is an orthopedic surgical emergency.
“Tongue-type” or “beak-type” calcaneal fractures are the most important to remember. Note their terms are often used interchangeably.
“Sleeve-type” fractures are PCT avulsions that can also threaten skin
Delays in definitive surgical repair can lead to soft tissue necrosis, amputation, and/or death.
CT scans should not delay time to orthopedics consultation or necessary transfers, though are important to guide management
Always: immobilization, application of a posterior leg splint, elevation (keep in mind risk of compartment syndrome), non-weight bearing status, and analgesia.
Use modified splint technique as demonstrated in Fig. 8 to alleviate pressure on skin of posterior heel
FURTHER READING
For a broader overview of calcaneal fractures, you will find an excellent Brown EM Blog post by Dr. Chana Rich from 2016 at this link. She reviews interpretation of lateral foot XRs (Bohler’s Angle, the Critical Angle of Gissane, double density sign), intra- vs extra-articular fractures, associated injuries, etc.
Author: James Tanch, MD, is a recent graduate of Brown Emergency Medicine
Faculty Reviewer: Michelle Myles, MD, is a clinician educator at Brown Emergency Medicine.
References
1) Snoap T, Jaykel M, Williams C, Roberts J. Calcaneus Fractures: A Possible Musculoskeletal Emergency. J Emerg Med. 2017;52(1):28-33.
2) AO Foundation [Internet]. Davos, Switzerland: AO Foundation. Extreme tongue-type (beak) fracture of the calcaneus body. 2010 [accessed 2020 May 26]. Available from: https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/calcaneous/extreme-tongue-type-beak-fractures/
3) Figure, Calcaneus Anatomy. Contributed by David R Davis MD. StatPearls. <https://www.ncbi.nlm.nih.gov/books/NBK430861/figure/article-18765.image.f1/>. Creative Commons: <http://creativecommons.org/licenses/by/4.0/>. Retrieved May 26, 2020.
4) Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK. Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma. 2008;22(7):439-445. doi:10.1097/BOT.0b013e31817ace7e
5) Gitajn IL, Abousayed M, Toussaint RJ, Vrahas M, Kwon JY. Calcaneal avulsion fractures: a case series of 33 patients describing prognostic factors and outcomes. Foot Ankle Spec. 2015;8(1):10-17. doi:10.1177/1938640014548323
6) Beavis RC, Rourke K, Court-Brown C. Avulsion fracture of the calcaneal tuberosity: a case report and literature review. Foot Ankle Int. 2008;29(8):863-866. doi:10.3113/FAI.2008.0000
7) Essex-Lopresti P. The mechanism, reduction technique, and results in fractures of the os calcis, 1951-52. Br J Surg. 1952;39(157):395-419
8) Lee SM, Huh SW, Chung JW, Kim DW, Kim YJ, Rhee SK. Avulsion fracture of the calcaneal tuberosity: classification and its characteristics. Clin Orthop Surg. 2012;4(2):134-138. doi:10.4055/cios.2012.4.2.134
9) Carnero-Martín de Soto P, Bautista-Enrique D, Gómez-Cáceres A, Rodríguez-León A, Bravo-Zurita MJ, Santos-Maraver MT. Avulsion Fractures of Posterior Calcaneal Tuberosity: Identification of Prognostic Factors and Classification. J Foot Ankle Surg. 2019;58(3):423-426. doi:10.1053/j.jfas.2018.09.002
10) Hsu RY, Lareau CR, Born CT. Novel posterior splinting technique to avoid heel ulcers. Orthopedics. 2013;36(1):31-32. doi:10.3928/01477447-20121217-03