FAST TRACK: Corneal Abrasions

FAST TRACK: Corneal Abrasions
CASE
A 32-year-old male presents to the emergency department (ED) with a chief complaint of eye pain after his toddler accidentally struck him in the eye while playing excitedly with a plastic toy set. He is complaining of foreign body sensation, redness, sensitivity to light, mild blurry vision and pain in his right eye. The left eye is unaffected. He does not wear contact lenses or glasses regularly.
DIAGNOSIS
Corneal abrasion

Figure 1 Corneal abrasion [4]
DISCUSSION
Eye-related diagnoses represent approximately 8% of total ED visits, and of those visits, approximately 45% are corneal abrasions [1]. A scratched cornea often causes significant discomfort, foreign body sensation, severe pain, eye erythema, light sensitivity, and photophobia. The majority of these types of abrasions are caused by nonpenetrating trauma to the corneal epithelium, usually due to minor accidental trauma by a poked finger, fingernail, tree branches, paper, makeup brushes, workplace debris, sports equipment, soap, detergents, etc [2]. Most patients with uncomplicated superficial corneal abrasions recover completely after 3 to 5 days [2].
It is vital to take a detailed history and perform a thorough examination when evaluating patients with eye complaints. When taking a history, it is imperative to ask about contact use, recent trauma, or exposure to possible metal or wood foreign bodies.
Topical anesthetics are helpful to facilitate eye examination. On exam, there is usually conjunctival injection. The upper and lower eyelids should be everted to visually inspect for presence of a foreign body. If there is concern for a foreign body despite a normal exam, consider orbital CT or MRI if foreign body is non-metallic. Fluorescein staining can help identify corneal defects. Apply 1 drop of fluorescein or use a fluorescein strip with topical anesthetic drop. Then examine the eye with a Wood’s lamp or slit lamp with cobalt blue light. There will be increased fluorescein uptake in areas with corneal defect.
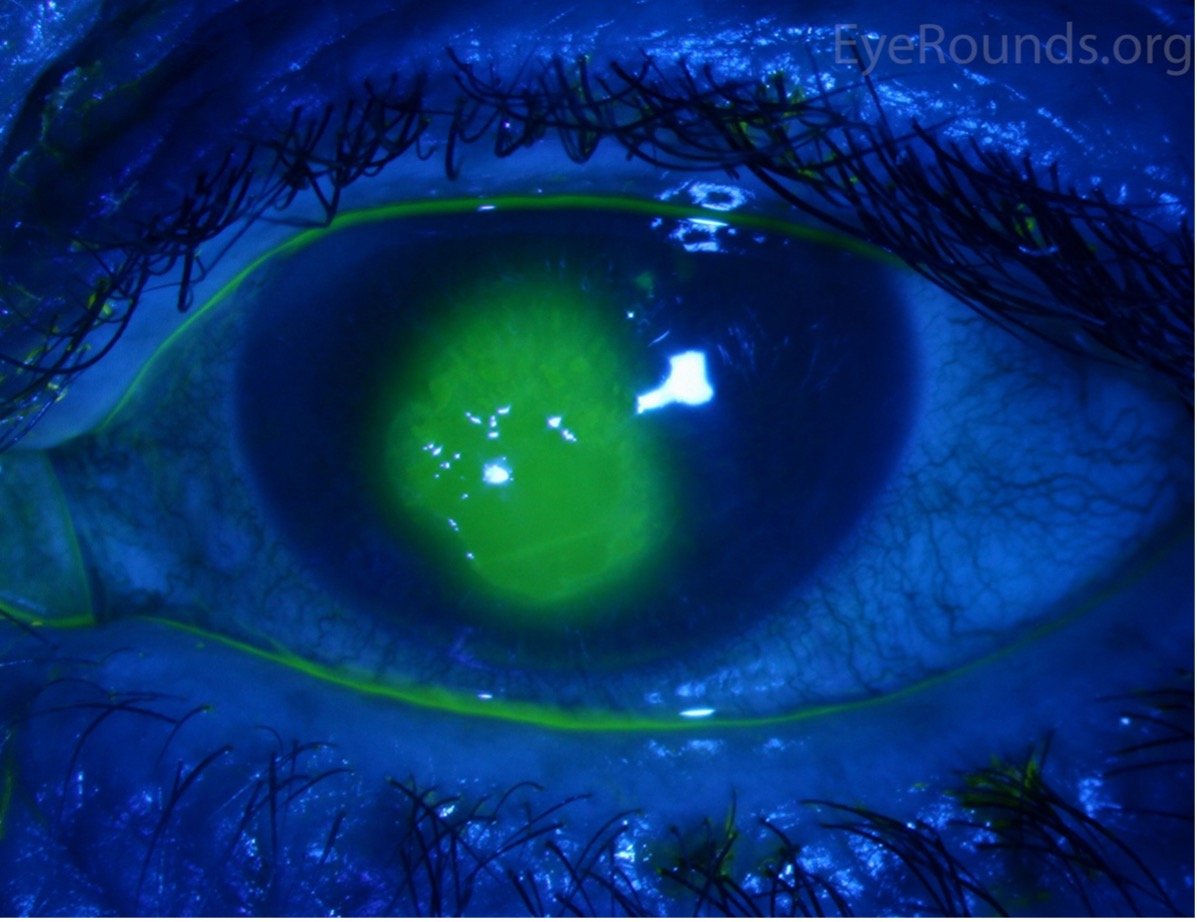
Figure 2 Increased fluorescein uptake in a corneal defect [5]
Signs that should prompt an immediate referral to ophthalmology include: an abnormally shaped pupil (could be a sign of globe rupture), evidence of hyphema or hypopyon, significant reductions in visual acuity, abnormal extraocular movements, corneal ulcers, branching/dendritic pattern on fluorescein exam (suggests possible herpes zoster ophthalmicus) [2][3].

Figure 3 A) Asymmetric pupil concerning for globe rupture [6] and B) dendritic pattern on fluorescein stain concerning for herpes ophthalmicus [5]
The goals of treatment of corneal abrasions are to prevent bacterial superinfection, speed healing, and to provide symptomatic relief to patients [1]. Management of uncomplicated corneal abrasions typically includes topical antibiotic treatment with either erythromycin ointment, ciprofloxacin 0.3% ophthalmic solution, ofloxacin 0.3% solution, or sulfacetamide 10% ophthalmic solution every 6 hours for 3-5 days. Antibiotic coverage should be expanded to cover pseudomonas in patients who wear contact lenses, and typically favor 3rd or 4th generation fluoroquinolones. The dosing schedule for contact-wearers is levofloxacin 0.5% solution 2 drops every 2 hours for 2 days, followed by 2 drops every 6 hours for 5 days, for a total of 7 days of treatment [3]. Minor abrasions (less than 4 mm) rarely require analgesia. Control mild to moderate pain with oral NSAIDs. Oral opioids can be considered for severe abrasions [2]. Prescribed topical anesthetics are contraindicated in patients with corneal injuries as repeated administration has been shown to delay corneal wound healing, mask worsening symptoms such as development of a corneal ulcer and can also be toxic to corneal epithelium [1].
TAKE-AWAYS
Corneal abrasions make up nearly half of ED visits for eye complaints, and are usually caused by minor non-penetrating trauma to the eye.
Collect a detailed history and perform a thorough exam to evaluate for foreign body, globe injuries, or signs of other etiologies of eye injury.
Treat uncomplicated corneal abrasions with topical antibiotic drops or lubricant and expand antibiotic choice to 3rd or 4th generation fluoroquinolones for contact-wearers. Oral NSAIDs may be used for pain. Prescribed topical anesthetics are contradicted.
Refer the following injuries for urgent ophthalmologic evaluation: globe injury, hyphema, hypopyon, abnormal extraocular movements, herpes ophthalmicus, or significantly reduced visual acuity.
Author: Lindsey Brown, MD is a current second year resident at Brown Emergency Medicine
Faculty Reviewer: Michelle Myles, MD is an attending physician at Rhode Island Hospital and Miriam Hospital.
REFERENCES
1. BH;, Ahmed F;House RJ;Feldman. “Corneal Abrasions and Corneal Foreign Bodies.” Primary Care, U.S. National Library of Medicine, 31 July 2015, pubmed.ncbi.nlm.nih.gov/26319343/. Accessed 20 Feb. 2024.
2. Domingo, Emilissa. “Corneal Abrasion.” StatPearls [Internet]., U.S. National Library of Medicine, 8 Jan. 2024, www.ncbi.nlm.nih.gov/books/NBK532960/. Accessed 20 Feb. 2024.
3. Donaldson, Ross et al. “Corneal Abrasion.” WikEM, 28 Aug. 2021, wikem.org/wiki/Corneal abrasion. Accessed 20 Feb. 2024.
4. Scott, Christina. “Corneal Abrasions.” Corneal Abrasions - American Association for Pediatric Ophthalmology and Strabismus, Mar. 2023, aapos.org/glossary/corneal-abrasions. Accessed 20 Feb. 2024.
5. Vislisel, Jesse. “Corneal Abrasion.” Atlas Entry - Corneal Abrasion, webeye.ophth.uiowa.edu/eyeforum/atlas/pages/corneal-abrasion/index.htm. Accessed 20 Feb. 2024.
6. Swaminathan, Anand. “Core Em: Traumatic Ocular Injuries.” emDOCs.Net - Emergency Medicine Education, 23 Sept. 2015, www.emdocs.net/core-em-traumatic-ocular-injuries/. Accessed 20 Feb. 2024.