Pectoralis Major Tendon Rupture: When the Pec Decides to Take a Major Break

case
A 40-year-old male with a past medical history of ulcerative colitis, anxiety, and depression presented to the emergency room with pain and swelling to the right pectoralis area for two days. The patient reported that he was doing bench presses of about 200 pounds two days ago when he felt some discomfort in his right chest, which he described as a tingling and tearing sensation. Over the subsequent 24 hours, he noted that there was some bruising to the affected area and as the day went on, he noticed that the ecchymosis was getting larger His pain was becoming constant, sharp/throbbing, moderate to severe, and worse with movement. He denied any numbness, pallor, or weakness in the right arm. However, he stated that when moving the right shoulder, he had significant pain throughout the shoulder and right arm.
Vital signs:
❖ Blood Pressure: 168/92
❖ Heart Rate:102
❖ Temperature: 99.3 °F
❖ Respiratory Rate: 20
❖ SpO2: 96%
Physical examination:
❖ Constitutional: well-developed, non-toxic, non-ill appearing. In no acute distress.
❖ Cardiac: regular rhythm, tachycardic. No murmurs, rubs, or gallops, 2+ radial pulse
bilaterally
❖ Pulmonary: clear to auscultation bilaterally
❖ Abdomen: soft, nontender, nondistended. No guarding, rebound, or rigidity.
❖ Musculoskeletal: ecchymosis, swelling, and tenderness throughout the anterior chest wall
extending into the proximal right upper extremity. Soft pectoral and upper extremity
compartments.
❖ Neurologic: intact motor and sensory function diffusely.
❖ Skin: warm, dry, and well perfused
Labs:
❖ CBC: WNL
❖ BMP:
➢ Potassium: 6.0
➢ BUN: 16
➢ Creatinine: 1.31 (baseline: 1.29-1.39)
➢ eGFR: 75 (baseline: 59-80)
❖ CPK: 4,500 down to 2,750
Imaging:
❖ CTA Right Upper Extremity With and Without IV Contrast: Subcutaneous stranding
associated with the right pectoralis, deltoid, and biceps muscles and axilla which could be
related to recent injury or infection in the appropriate setting.
hospital course
The patient was admitted for further management of his rhabdomyolysis. He received Lokelma
for his hyperkalemia and approximately three liters of fluids total. He subsequently underwent an
MRI of his chest without IV contrast that showed a full-thickness tear of the right distal
pectoralis major tendon with tendon retraction and hematoma formation.
diagnosis
1. Traumatic rhabdomyolysis
2. Full-thickness tear of the right distal pectoralis major tendon with tendon retraction
discussion
Ruptures of the pectoralis major muscle and tendon, although previously uncommon, have been on the rise due to increased interest in health, fitness, and exercise. The typical patient demographic for this condition is usually young, active, and in good health. Age ranges can vary between 15 to 91, but male athletes ages 20 to 40 make up the majority of cases. The most commonly associated activities that can result in pectoralis muscle tear include weight-lifting, with bench press being the most common inciting activity, followed by water-skiing, football, wrestling, parallel bar dips, ice hockey, and windsurfing. Anabolic steroid use also plays a role in this condition. Patients may sometimes go misdiagnosed as a strain or sprain potentially leading to a disabling injury if not managed appropriately [1].
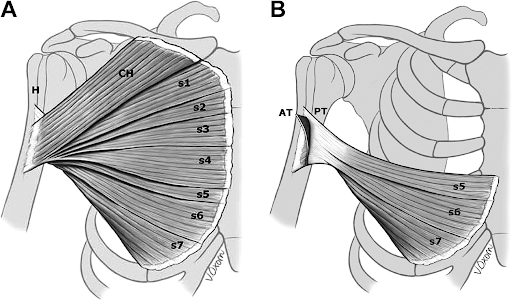
The main functions of the pectoralis major include adduction, internal rotation, and flexion of the humerus. It is primarily innervated by the medial (C8-T1) and lateral (C5-C7) pectoral nerves that arise from the brachial plexus. The pectoralis major has a complex musculotendinous make-up that consists of a clavicular head and a sternal head. The clavicular head comes from the medial half of the clavicle while the larger sternal head, which accounts for nearly 80% of the total muscle volume, arises from the ribs 2-6, the costal margin of the sternum, and the external oblique aponeurosis. The sternal head can be further subdivided into 7 additional segments as seen in the diagram below. [1, 2, 3].
Diagnosis of a pectoralis major muscle tendon tear is typically obtained by the history and physical. There is often a sudden pain at the medial aspect of the upper arm associated with a “pop” felt by the patient. This most commonly occurs with eccentric contraction during strenuous activity. Physical examination may reveal ecchymosis over the anterolateral chest wall and upper arm along with a variable degree of swelling. Loss of the anterior axillary fold with an asymmetric muscle outline that is retracted medially is a useful diagnostic feature although this may be partially obscured by soft tissue swelling in the acute phase. Ultrasound may be helpful when the diagnosis is in doubt or when time to MRI is delayed; however, MRI is the imaging modality of choice [2].
A potential, yet uncommon, complication of a pectoralis major tendon rupture is traumatic rhabdomyolysis. The incidence of rhabdomyolysis increases when complete tendon tears occur, larger muscle masses are present, and with direct muscle belly involvement. The most common muscle groups to experience traumatic rhabdomyolysis are the larger muscles of the thighs, calves, and lower back [4]. A lower threshold to obtain labs should be considered if the above criteria are present.
Surgical repair under general anesthesia is required in young, healthy patients with acute tendon ruptures. Conservative management is typically indicated in elderly patients, partial tendon tears, and muscle belly ruptures. When surgical and conservative management were compared, patients who underwent operative fixation fared better than those who did not [3, 5].
case resolution
The patient’s potassium improved and his CPK continued to downtrend while inpatient after IV fluid therapy. He was ultimately discharged from the hospital and referred to orthopedics for outpatient repair of his pectoralis major tendon rupture.
take-aways
Pectoralis major tendon ruptures are becoming more common with increased interest in physical fitness and exercise.
MRI is the imaging modality of choice to make the diagnosis of a pectoralis major tendon rupture.
Rhabdomyolysis is a potential complication of pectoralis major tendon injury. Have a lower threshold to obtain labs when larger muscle groups are affected.
Prompt recognition and early referral to orthopedic surgery for operative repair drastically improves patient outcomes.
AUTHOR: Dylan Perez, DO, is a second-year emergency medicine resident at Brown Emergency Medicine Residency
FACULTY REVIEWER: Frederick Varone, MD, is an attending physician at Rhode Island Hospital and an Assistant Professor of Emergency Medicine.
REFERENCES
1. Hasegawa, Kohei, and Joel M Schofer. [Internet] “Rupture of the Pectoralis Major: A Case Report and Review - Sciencedirect.” Science Direct, 10 Feb. 2010. [Accessed 12 April 2025]. Available from: www.sciencedirect.com/science/article/abs/pii/S0736467908003168.
2. Butt, Usmann, et al. [Internet] “Pectoralis Major Ruptures: A Review of Current Management.” Journal of Shoulder and Elbow Surgery, Mosby, 1 Jan. 2015. [Accessed 12 April 2025]. Available from: www.sciencedirect.com/science/article/abs/pii/S1058274614006314.
3. Bodendorfer, Blake M, et al. [Internet] “Treatment of Pectoralis Major Tendon Tears: A Systematic Review and Meta-Analysis of Operative and Nonoperative Treatment.” Orthopaedic Journal of Sports Medicine, U.S. National Library of Medicine, 6 Feb. 2020. [Accessed 13 April 2025]. Available from: pubmed.ncbi.nlm.nih.gov/32083144/.
4. Khans, F Y, et al. [Internet] “Rhabdomyolysis: Review of the Literature.” Neuromuscular Disorders, Elsevier, 21 May 2014. [Accessed 2 June 2025]. www.sciencedirect.com/science/article/pii/S096089661400131X.
5. Merolla, Giovanni, et al. [Internet] “Pectoralis Major Tendon Rupture. Surgical Procedures Review.” Muscles, Ligaments and Tendons Journal, U.S. National Library of Medicine, 10 Sept. 2012. [Accessed 13 April 2025]. Available from: pmc.ncbi.nlm.nih.gov/articles/PMC3666500/.