Point-of-Care Ultrasound in Early Pregnancy

…Emergency physician proficiency in POCUS in early pregnancy could improve patient flow and satisfaction…
Background
Many patients present to the emergency department with abdominal pain or vaginal bleeding in the first trimester of pregnancy, often without a prior ultrasound to confirm an intrauterine pregnancy (IUP). For these patients, it is essential to take steps to rule out an ectopic pregnancy via ultrasound as a ruptured ectopic pregnancy can be life-threatening.
Emergency physicians can perform this ultrasound evaluation at the bedside without sending the patient for a comprehensive pelvic ultrasound in most cases. A meta-analysis showed that emergency physician point-of-care ultrasound (POCUS) is 99.3% sensitive for identifying an IUP (1). As is the case with most POCUS examinations, outcomes are operator-dependent and sensitivity improves with experience. Another study found that sensitivity for identifying an IUP was highest when the operator had done 40 or more exams (2).
Patients who underwent POCUS examination for identification of an IUP had a length of stay in the emergency department that was over an hour shorter than those who went for comprehensive ultrasound (3). Emergency physician proficiency in POCUS in early pregnancy could improve patient flow and satisfaction.
Technique
Both transabdominal ultrasound and transvaginal ultrasound can be used to evaluate early pregnancy, with each having certain pros and cons. For example, structures can be seen at an earlier gestational age via transvaginal ultrasound and patients with larger body habitus may have poor candidacy for transabdominal ultrasound in the first trimester.
Below are general guidelines for when various structures can be seen on transabdominal versus transvaginal ultrasound:
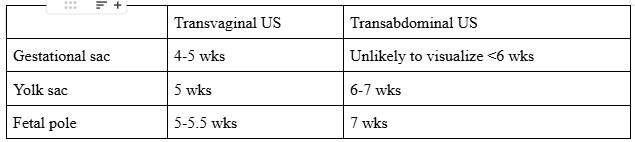
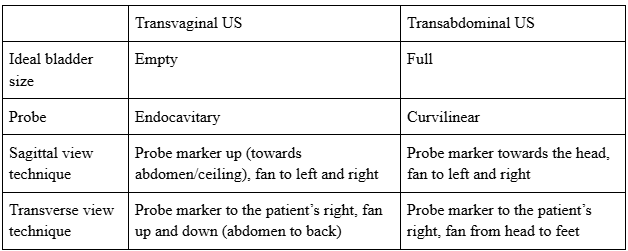
The table below outlines basic tips and tricks for pelvic ultrasound technique:
Structures to Identify
The gestational sac appears as an anechoic, round structure with an echogenic border.
A key pitfall is the pseudogestational sac, which may resemble a gestational sac but lacks a yolk sac within it. A pseudogestational sac does not confirm an IUP and can be seen in patients with ectopic pregnancy.
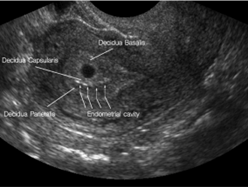
The double decidual sign, characterized by two concentric echogenic rings (one surrounding the gestational sac and one lining the uterine cavity) can help confirm that the gestational sac is actually within the uterus as shown below.
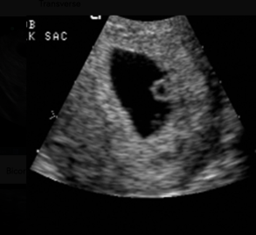
The yolk sac appears as an additional anechoic round structure with an echogenic border located within the gestational sac as in the photo below. Identification of a yolk sac definitively confirms an intrauterine pregnancy.
The fetal pole is a thickening along the wall of the yolk sac and corresponds to the early fetus. When it is developed enough (typically around 5 mm in length) the fetal pole will show a ‘cardiac flicker’.

Measure the Fetal Heart (FH)
To measure the fetal heart rate, first locate the fetal heart on ultrasound. Once identified, place the M-mode cursor directly over the location of the heartbeat and activate M-mode. Then, open the OB measurements menu and place the cursors over one or two cardiac cycles (machine dependent) to calculate the fetal heart rate.
Dating of an Intrauterine Pregnancy (IUP)
If the pregnancy is less than 12 weeks, crown-rump length (CRL) should be used. This typically dates automatically on the ultrasound machine, but gestational age can also be calculated manually using the following formula:
CRL in millimeters + 42 = gestational age in days
Between 12–20 weeks, biparietal diameter can be used for dating and in the second trimester. Femur length may also be used.
Interpretation
An intrauterine pregnancy (IUP) can be definitively diagnosed when multiple criteria are met. There must be a gestational sac present with either a yolk sac or a fetal pole, and the gestational sac must clearly be inside the uterus.
In addition, the endomyometrial mantle—the distance from the gestational sac to the outer edge of the myometrium—should measure at least 5–7+ mm. If the endomyometrial mantle is less than 5 mm, the pregnancy could represent an interstitial ectopic pregnancy, which can continue to grow and become very dangerous if rupture occurs.
Importantly, a fetal heart rate is not required to diagnose an intrauterine pregnancy.
Identifying an IUP is usually sufficient to rule out an ectopic pregnancy. A heterotopic pregnancy—the presence of both an IUP and an ectopic pregnancy at the same time. The exception being in the setting of fertility treatments, where it may occur as frequently as 1 in 100 pregnancies.
An ectopic pregnancy can be diagnosed when a gestational sac with either a yolk sac or a fetal pole is identified outside of the uterus. More commonly, ectopic pregnancy is suspected based on the absence of an IUP, rather than by direct visualization of a definitive ectopic pregnancy.
If there is no definitive IUP on ultrasound, this may represent either an ectopic pregnancy or a very early intrauterine pregnancy. This is called a pregnancy of unknown location (PUL).
Next Steps
If an IUP is identified, the patient can typically be discharged with routine obstetric follow-up.
If an IUP is not identified, a comprehensive pelvic ultrasound and a quantitative β-hCG should be ordered. A comprehensive ultrasound may identify an intrauterine or ectopic pregnancy. If the ultrasound remains inconclusive, the patient will require close follow-up with serial β-hCG levels and repeat ultrasounds until the pregnancy is confirmed as intrauterine or ectopic and managed accordingly.
References:
Stein JC, Wang R, AdlerN, et al. Obstetrics and gynecology/original research: emergency physician ultrasonography for evaluating patients at risk for ectopic pregnancy: a meta-analysis. Annals of Emergency Medicine 2010; 56(6):674–83.
Jang, T. B., Ruggeri, W., Dyne, P., & Kaji, A. H. (2010). Learning curve of emergency physicians using emergency bedside sonography for symptomatic first‐trimester pregnancy. Journal of ultrasound in medicine, 29(10), 1423-1428.
Blaivas, M., Sierzenski, P., Plecque, D., & Lambert, M. (2000). Do emergency physicians save time when locating a live intrauterine pregnancy with bedside ultrasonography?. Academic Emergency Medicine, 7(9), 988-993.
Chiang, G., Levine, D., Swire, M., McNamara, A., & Mehta, T. (2004). The intradecidual sign: is it reliable for diagnosis of early intrauterine pregnancy?. AJR. American journal of roentgenology, 183(3), 725–731.
The POCUS Atlas. (n.d.). The POCUS Atlas. https://www.thepocusatlas.com/