Utility of POCUS in Evaluating for Pulmonary Embolism
CASE
A 58-year-old woman with a past medical history significant for hypertension and hyperlipidemia presents to the Emergency Department with 3 days of dyspnea. She also endorses non exertional pleuritic chest pain, chills, and malaise that started on the morning of her presentation. Vital signs were notable for tachycardia of 110 beats per minute and an oxygen saturation of 93% on room air, but were otherwise normal. Physical exam revealed clear lung fields bilaterally and was otherwise unremarkable.
DIAGNOSIS
The patient was ordered for a Chest CT Angiogram (CTA) to confirm the diagnosis, but due to high patient volume in the department, the study takes three hours to complete. The CT eventually results and confirms the diagnosis of pulmonary embolism (PE), showing clot burden bilaterally in the pulmonary vasculature. The patient is started on heparin and admitted for new oxygen requirement and further anticoagulation.
DISCUSSION
Pulmonary embolism is a diagnosis that carries significant morbidity and mortality when not properly recognized and treated, making early diagnosis important. [1] With busy emergency departments and long wait times for CT studies, it may be prudent to ask the question: Is there utility in Focused Cardiac Ultrasound (FOCUS) in early diagnosis of PE? A recent meta-analysis showed that in patients with clinical suspicion for PE, but without vital sign abnormalities, right heart strain on FOCUS had a sensitivity of 53% (95% CI, 45%-61%) and a specificity of 83% (95% CI, 74%-90%) in diagnosis of PE. [2] This data might lead one to believe that FOCUS has little clinical utility in the diagnosis of PE. We can postulate, however, that in patients with a PE and clot burden that is significant enough to cause vital sign changes, there would be a higher probability of right heart strain. [1] In this population, it is reasonable to ask whether FOCUS could play a role in the early diagnosis or in ruling out of pulmonary embolism. Daley et. al tried to answer this exact question in 2019 when they published a study looking at the sensitivity of FOCUS in evaluating patients with suspected PE and tachycardia or hypotension. They used the following measures to evaluate for right heart strain: McConnell’s sign, Tricuspid Annular Plane Systolic Excursion (TAPSE), septal flattening, right ventricular enlargement, and tricuspid regurgitation. [3] The FOCUS exam was considered positive if any one of these five measures were present.
ULTRASOUND IMAGES
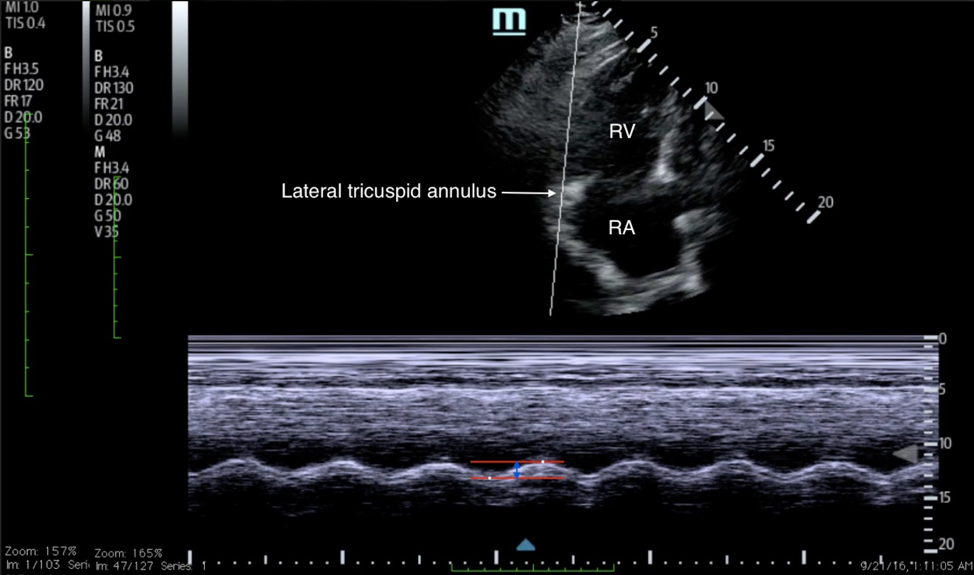
Figure 1: Tricuspid Annular Plane Systolic Excursion (TAPSE) is a measure used to estimate right ventricular function. A value of 2.0 cm or greater is considered normal, anything less than this can be considered evidence of right heart dysfunction. [4]
Figure 2. McConnell’s Sign is defined as hypokinesis of the right ventricular wall with apical sparing. It is associated with acute right ventricular dysfunction, often seen with pulmonary embolism. [5]
CONCLUSION
The study results showed that in patients with heart rate (HR) greater than 110, the sensitivity of FOCUS for PE was 100% (95% CI = 88% to 100%). In patients with HR greater than 100, the sensitivity was 92% (95% CI = 78%-98%). [3] These results suggest that FOCUS performed by emergency physicians has the potential to rule out pulmonary embolism in patients with which there is clinical suspicion and vital sign abnormalities. Patients with unstable vital signs should not be sent for a CT study, so being able to rule out critical diagnoses with ultrasound at the bedside offers great value.
TAKE-AWAYS
FOCUS has limited clinical utility for the evaluation of PE in stable patients
In a patient with suspicion for PE AND HR >110, FOCUS has a high sensitivity which may be useful in ruling out PE
Tricuspid Annular Plane Systolic Excursion (TAPSE), was the most sensitive measure of right heart strain when compared to the other components of the FOCUS exam in evaluation for PE
McConnell’s sign was the most specific component of the FOCUS exam for PE
AUTHOR: Benjamin Hagan, MD is a first year emergency medicine resident at Brown University/Rhode Island Hospital.
FACULTY REVIEWER: Kristin Dwyer, MD is the Director of Ultrasound Division of Brown Emergency Medicine
REFERENCES
Tintinalli, Judith E.,, et al. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. Eighth edition. New York: McGraw-Hill Education, 2016. 434-438.
Fields J, Davis J, Girson L, et. al. Transthoracic Echocardiography for Diagnosing Pulmonary Embolism: A Systematic Review and Meta-Analysis. J Am So Echocardiograph. 2017. 30: 714-23.e4.
Daley J, Dwyer K, Grunwald Z, et. al. 1. Increased Sensitivity of Focused Cardiac Ultrasound for Pulmonary Embolism in Emergency Department Patient with Abnormal Vital Signs. SAEM Journal. 2019. 26(11). 1213-1220.
Journal of Education & Teaching in Emergency Medicine [Internet]. Irvine: Journal of CORD. Tricuspid Annular Plane Systolic Excursion (TAPSE) in a Patient with Pulmonary Emboli. 2016 [accessed 2020 Dec 02]. Available from: https://jetem.org/tapse/.
The POCUS Atlas [Internet]. Kings County Emergency Medicine. McConnell’s Sign-Pulmonary Embolism. 2019 [accessed 2020 Dec 02]. Available from: https://www.thepocusatlas.com/bb-echo.