Emergency Department Application of J-splints to Temporize Pediatric Femur Fractures
CASE
A four-year-old female with no medical history presented to the emergency department with right leg pain and refusal to walk after falling while in her father’s arms. She was being carried by her father down a flight of outdoor concrete stairs when he slipped on black ice and her leg struck the ground. The patient refused to walk after the fall and her mother noted that her leg had been “cracking” since the accident.
On exam, the patient was tachycardic for age to 140 and obese for age (25.5kg). Otherwise, vitals were unremarkable. Exam notable for an obese appearing toddler without any evidence of head trauma. She was lying in a frog leg position and hesitant to move her right leg. She had an obvious deformity and significant tenderness of the right mid-thigh. The overlying skin was intact with a normal neurovascular exam of the extremity.

Figure 1. Two View Right Femur X-rays.
DIAGNOSIS
Right transverse mid-shaft femur fracture
DISCUSSION
Pediatric femur fractures account for just under 2% of all pediatric fractures and are the most common reason for pediatric hospitalization for an orthopedic injury. [1] The etiology of femur fractures in children varies by age group but includes mechanisms such as falls, motor vehicle accidents, sports injuries, and non-accidental trauma (NAT). The most common cause of femur fractures in children less than one year of age is NAT and some have suggested that NAT is prevalent in patients up to 5 years of age. [1] Transverse fractures are also more predictive of NAT than spiral fractures. [2] It is important for the emergency physician (EP) to maintain a high index of suspicion for NAT with this injury pattern.
Various operative and nonoperative treatment options for pediatric femur fractures exist. Classic nonoperative treatments include a Pavlik harness, spica casting, and traction with delayed spica casting. Operative options include the use of flexible intramedullary nails, plate fixation, rigid nail fixation, and external fixation. While many factors go into the choice treatment these are decisions left to the orthopedists which will be definitively managing these patients.
In the emergency department (ED) the goal for fracture temporization is often hemorrhage control, fracture stabilization, and pain relief while awaiting definitive management. Several methods for stabilization including skeletal traction, skin traction, traction splinting, posterior splinting, and J-splinting have been described. [3] Skeletal traction provides excellent reduction but is associated with the risk for substantial morbidity and is not performed without the assistance of the orthopedics team. Skin traction is limited by the amount of force that can be applied compared to skeletal traction and makes transfers difficult. Traction splints are commonly used in the field and in adult patients but should not be used for more than six hours due to the risk of skin breakdown and peroneal nerve palsy. [3] Long posterior leg splints are easy to apply but are largely ineffective at stabilization as they provide little angular correction of proximal or midshaft fracturs. [3]
A relatively new splint, the J-splint, is a rapid and easy to apply alternative. First described by Daniels et al., this technique is indicated for any fracture in children too large for a Pavlik harness up to approximately 100lbs (for patients less than 6 months of age Pavlik harness is definitive management). [4] A J-splint can be left in place until the patient receives definitive management approximately 24-48 hours after the injury and has the benefit of immobilizing knee, tibia, and foot injuries. [4] They also note that a J-splint can be performed in the field, in hospitals and clinic without the resources to perform skeletal or skin traction and can be used in mass casualty scenarios. [4]
While J-splinting performs well in coronal and sagittal reduction, J-splinting is ineffective in preventing fracture shortening, therefore selection of this technique will be contingent on the morphology of the fracture. [4] If patients have multiple injuries that preclude them from definitive management within 24-48 hours skeletal traction or skin traction should be used for adequate axial traction. [4]
Technique for Application of a J-splint for Pediatric Femur Fractures as Described by Daniels et al. [4]
Adequate analgesia and anxiolysis should be obtained prior to splinting. One or two assistants are used based on available resources. Plaster is the preferred splinting material due to its ability to retain molding.
Use 4-inch plaster for children <50 lb and 6-inch plaster for children >50 lb using 8-10 layers.
Measure the length of the plaster using the contralateral leg from the axilla down the lateral torso and leg around the foot and up the medial contralateral leg to the groin.
At least 5 layers of cast padding should be laid over the top of the plaster and additional padding should be used especially in the axilla, groin, lateral and medial malleoli.
An assistant holds the fractured limb in anatomic alignment with axial traction.
Elastic wrap (size varies based on age) beginning at the foot should be applied so that it is tight enough to hold the splint in place but loose enough to avoid compression of soft tissue.
The wrap should be continued to include the torso and ipsilateral axilla as shown in Figure 2.

Figure 2: Pictographic representation of J-splint. Red outline indicates plaster mold.
CASE RESOLUTION
A J-splint was applied as described above for closed reduction and splinting of the patient’s right lower extremity. Post reduction radiographs were obtained which showed improved angulation from the original film (Figure 3). The patient exhibited better pain control after the splint was applied and tolerated the splinting well without complication.
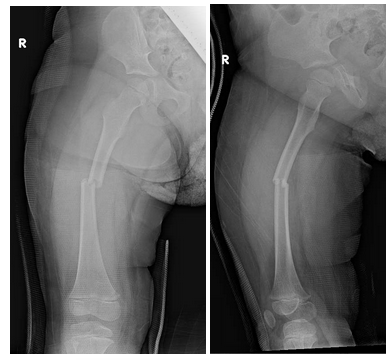
Figure 3. Post reduction X-rays in J-Splint.
Ultimately the decision to treat with elastic intramedullary nailing versus more traditional spica casting was made by the orthopedist and the family given the displacement, transverse nature of the fracture, and the patient’s body habitus.
The surgery was successfully completed without complication and was discharged the following day with orthopedics follow-up.
TAKE-AWAYS
J-splinting in the emergency setting for patients greater than 6 months of age and less than 100 lbs with femoral fractures can provide stabilization, pain control, and good coronal and sagittal reduction until definitive management can be obtained (24-48 hours after injury).
J-splinting is ineffective in preventing fracture shortening.
Splint material should have significant padding especially over the groin, axilla, lateral, and medial malleoli.
J-splints are only used as temporizing measures and are not used for the definitive management of pediatric femur fractures.
Maintain a high index of suspicion for NAT in pediatric femur fractures (especially if transverse and before the patient is of walking age).
AUTHOR: Eric Ebert MD, is a first-year resident at Brown University/Rhode Island Hospital
FACULTY REVIEWER: Jared Anderson MD
REFERENCES
American Academy of Orthopaedic Surgeons. Treatment of Pediatric Diaphyseal Femur Fractures Evidence-Based Clinical Practice Guideline. www.aaos.org/pdffcpg. Published March 23, 2020.
Murphy R, Kelly DM, Moisan A, Thompson NB, Warner WC Jr, Beaty JH, Sawyer JR. Transverse fractures of the femoral shaft are a better predictor of nonaccidental trauma in young children than spiral fractures are. J Bone Joint Surg Am. 2015 Jan 21;97[2]:106-11. doi: 10.2106/JBJS.N.00664. PMID: 25609436.
Ritterman, Scott, Daniels, Alan, Kane, Patrick, Eberson, Craig, Born, Christopher. J-Splint Use for Temporizing Management of Pediatric Femur Fractures: A Review of 18 Cases. Pediatr Emerg Care. 2014;30(8):516-520. doi:10.1097/PEC.0000000000000181.
Daniels, A., Kane, P., Eberson, C., & Born, C. (2012). Temporizing management of pediatric femur fractures using J-splints. Orthopedics, 35 9, 773-6.