CLUNK! I Can’t Move My Foot

“A 13-year-old otherwise healthy female presents to the emergency department for right knee pain after an injury while playing basketball.”
Case
A 13-year-old otherwise healthy female presents to the emergency department for right knee pain after an injury while playing basketball. She states that she was dribbling the ball and attempted to pivot, when she felt a “pop” in her right knee. She fell to the ground with immediate right knee pain and denies any other injuries.
When she arrives at the emergency department, she endorses extreme pain, as well as paresthesia, in her right leg. Her vital signs are unremarkable. Her physical exam is notable for a visible deformity of the right knee with edema. She is diffusely tender throughout the knee, as well as the distal femur and proximal tibia and fibula. Active range of motion of the right foot, knee, and hip is limited by pain. Dorsalis pedis and posterior tibial pulses are found on Doppler. The right ankle-brachial index (ABI) is calculated to be 0.74 compared to the contralateral side of 0.98. In addition, the patient is presenting with diminished sensation over the peroneal and tibial nerve distributions.
An x-ray is performed that demonstrates an anterior-medial dislocation of the right knee. The patient’s knee is reduced and, afterwards, the patient’s pain significantly improves. Her ABI on the right extremity improves from 0.74 to 0.98, matching the contralateral limb. However, she continues to have paresthesia in the dorsum of her foot and has difficulty dorsiflexing her right foot. Post-reduction films of her right knee demonstrates a fracture-dislocation of her right knee.
A CT angiogram is deferred due to restoration of her ABI. An MRI is completed that demonstrates a fracture-dislocation, complete ACL tear, partial PCL and MCL tear, posterolateral corner injury, biceps femoris tear, fractures of the tibial plateau and femoral condyle, and lateral subluxation of the patella with partial tear of the patellar tendon. The patient is admitted to the orthopedics service.
Diagnosis
This patient suffered an anterior knee dislocation. Secondary to the injury, she sustained severe damage to the peroneal and tibial nerves. She also had multiple soft tissue injuries and associated fractures.
Discussion
A traumatic knee dislocation is an orthopedic emergency due to the high risk of damage to the neurovascular structures coursing through the knee [1,2]. Although a knee dislocation is a rare injury and accounts for only 0.02% of orthopedic injuries, it requires prompt intervention in the emergency department [3]. There are various mechanisms that can lead to this injury. High-energy mechanisms include motor vehicle crashes, often involving dashboard injuries where an axial load is placed on a flexed knee. In addition, crush injuries or falls from heights can also cause knee dislocations [1]. With regards to low-energy mechanisms, knee dislocations can occur from walking or athletic injuries, especially in obese patients [1,4]. Anterior dislocations (Figure 1) tend to be the most common, with an incidence of 30% to 50%, closely followed by posterior dislocations (Figure 2), which account for 30% to 40% [1]. A simple way of discerning anterior versus posterior on x-ray is by looking at the distal appendage (the tibia and fibula) and seeing what direction it is displaced.
While soft tissue injuries are associated with knee dislocations, the most concerning injuries are those to the neurovascular structures. Anterior dislocations are associated with more nerve injuries, specifically the peroneal nerve, while posterior dislocations tend to be associated with popliteal artery damage [1,5]. Peroneal nerves tend to present with foot drop or an inability to dorsiflex the foot whereas popliteal artery injuries tend to present with diminished dorsalis pedis or posterior tibialis pulses.
When patients present to the emergency department, there may or may not be an obvious deformity, as nearly 50% of dislocated knees may spontaneously reduce on their own [1]. Regardless, if there is any suspicion for a knee dislocation or if the diagnosis is confirmed on x-ray, it is imperative to conduct a thorough neurovascular exam. Reduction should be considered if there is any concern for neurovascular injury, and the knee must be immobilized ideally in 20 degrees of flexion [5,6]. It is important to check for sensation and motor function of the peroneal and tibial nerves, though peroneal nerve palsies tend to be more common [3]. It is also necessary to check posterior tibialis and dorsalis pedis pulses. An ABI should be calculated, as this can direct management. If patients have an ABI >0.9, they may be serially monitored for vascular status and compartment syndrome. If patients have an ABI <0.9 after reduction, further imaging such as CT angiography should be considered [7]. Prompt emergency department management can direct long-term outcomes, as patients treated surgically for vascular injuries within 8 hours have had significantly lower rates of amputation (11%) compared to those operated on after 8 hours (86%) [8].
In the case of this patient, she suffered an anterior knee dislocation with complete transection of both the peroneal and tibial nerves, which is consistent with the literature suggesting that anterior dislocations are associated with more nerve injuries. While she did not suffer from vascular compromise, her ABI increased from 0.74 to 0.98 after reduction, suggesting that she may have had some vascular compression from the dislocation. Concomitant vascular and nerve damage from a knee dislocation is a rare complication [9].
The management of this patient in the emergency department illustrates the importance of prompt intervention for knee dislocations. Her perfusion was restored after a reduction within 1-2 hours of her injury, further reducing her risk of an amputation. However, she still required urgent surgery for her transected peroneal and tibial nerves.
There is oftentimes collaboration between emergency medicine providers and orthopedists, as many of these patients require admission and/or close follow-up. In resource-limited settings where orthopedists may not be in-house, it is imperative for emergency medicine providers to identify and stabilize knee dislocations early on, while also being aware of the high risk of neurovascular complications.
CASE Resolution
The patient underwent a surgery to repair several of the soft tissue structures in her knee, followed by a second surgery to repair the completely severed peroneal and tibial nerves. Her sensation and motor function improved. The patient was discharged on hospital day 9 with possible ACL and PCL repair in the future.
Take Away Points
· Knee dislocations are orthopedic emergencies
· If there is concern for dislocation, reduce and immobilize the joint, it if it has not already spontaneously reduced
· Maintain high clinical suspicion for neurovascular injury, especially of the peroneal nerve and popliteal artery
· Involve orthopedics early to ensure timely surgical intervention and optimal outcomes

Figure 1: Anterior Dislocation (distal appendage is anteriorly displaced)
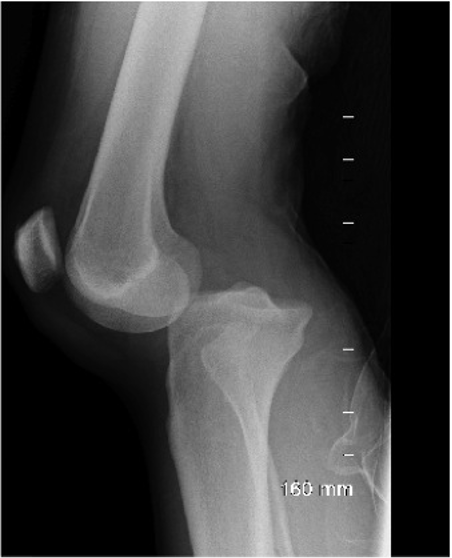
Figure 2: Posterior dislocation (distal appendage is posteriorly displaced)
Author: Prassana Kumar, MD is a second-year emergency medicine resident at Brown Emergency Medicine Residency.
Faculty Reviewer: Kristina McAteer, MD is an attending emergency medicine physician at Rhode
Island Hospital and Newport Hospital.
Bibliography
1. https://www.orthobullets.com/trauma/1043/knee-dislocation
2. O'Malley MP, Pareek A, Reardon P, Krych A, Stuart MJ, Levy BA. Treatment of Peroneal Nerve Injuries in the Multiligament Injured/Dislocated Knee. J Knee Surg. 2016;29(4):287-292. doi:10.1055/s-0035-1570019
3. Lachman JR, Rehman S, Pipitone PS. Traumatic Knee Dislocations: Evaluation, Management, and Surgical Treatment. Orthop Clin North Am. 2015;46(4):479-493. doi:10.1016/j.ocl.2015.06.004
4. Folt J, Vohra T. Low-velocity knee dislocation in the morbidly obese. Am J Emerg Med. 2012;30(9):. doi:10.1016/j.ajem.2011.12.031
5. Seroyer ST, Musahl V, Harner CD. Management of the acute knee dislocation: the Pittsburgh experience. Injury. 2008;39(7):710-718. doi:10.1016/j.injury.2007.11.022
6. Knutson T, Bothwell J, Durbin R. Evaluation and management of traumatic knee injuries in the emergency department. Emerg Med Clin North Am. 2015;33(2):345-362. doi:10.1016/j.emc.2014.12.007
7. Boyce RH, Singh K, Obremskey WT. Acute Management of Traumatic Knee Dislocations for the Generalist. J Am Acad Orthop Surg. 2015;23(12):761-768. doi:10.5435/JAAOS-D-14-00349
8. Green NE, Allen BL. Vascular injuries associated with dislocation of the knee. J Bone Joint Surg Am. 1977;59(2):236-239.
9. Massara M, Prunella R, De Caridi G, et al. Traumatic Anterior Knee Dislocation with Popliteal Artery Injury: The Importance of a Prompt Diagnosis and Treatment to Obtain Lower Limb Salvage. Ann Vasc Surg. 2017;43:309.e1-309.e3. doi:10.1016/j.avsg.2016.12.020