Septic Arthritis vs. Transient Synovitis: A Clinical Guide for the ED

…the differential diagnosis is broad—ranging from benign to limb- or life-threatening…
Introduction
Pediatric limp is a common and often anxiety-inducing presentation in the Emergency Department (ED), with an incidence of approximately 4 per 1000 visits
While the differential diagnosis is broad—ranging from benign to limb- or life-threatening—two key considerations in the atraumatic child are septic arthritis and transient synovitis. This blog post will focus on differentiation and evaluation of septic arthritis and transient synovitis. Differentiating these entities rapidly is critical, as septic arthritis carries the risk of joint destruction and systemic sepsis, whereas transient synovitis is self-limited.
History
Obtaining a comprehensive history is crucial for helping to differentiate between transient synovitis and septic arthritis. Pertinent information to elicit in the history include:
History of trauma
Use of medications and any improvement noted
Known tick exposure or exposure outdoors in endemic area
Concerning symptoms such as weight loss, lethargy, and/or pallor
History of recent illnesses
Fevers
Examination
A structured exam is essential. While observation of gait can be useful, many children often do not want to ambulate. Key exam findings include:
Joint evaluation: Swelling, erythema, warmth, effusion, or painful limitation of range of motion.
Systemic signs: Fever, irritability, lymphadenopathy, or hepatosplenomegaly, suggesting rheumatologic or infectious etiologies.
Localization clues:
Carefully examine all joints of the lower extremity in attempt to localize involved joints as children often have difficulty localizing their pain
Palpate long bones in attempt to identify if pain can be localized to a joint or long bone
Flexion Abduction External Rotation (FABER) test → may indicate sacroiliac joint involvement.
Psoas sign → possible psoas abscess or appendicitis.
Red flags: Inability to bear weight and pain with passive motion should raise concern for the possibility of septic arthritis.
Imaging and Diagnostics
Labs
Complete blood count (CBC), Erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP): Elevated WBC and inflammatory markers can support septic arthritis but are not diagnostic.
Blood cultures: Yield is variable but may guide therapy. If septic arthritis is a possibility, consider drawing a blood culture at the time of intravenous line placement as it should be obtained in a sterile manner.
Kocher Criteria (for suspected septic arthritis of the hip)
Non-weight bearing status
ESR > 40 mm/hr
Fever > 38.5°C
WBC > 12,000/mm³
The probability of septic arthritis increases with each criterion, but limitations exist—particularly outside of the hip. The criterion each count for one point, for a total possibility of 4 points. One point corresponds to a 3% probability of septic arthritis, 2 points is a 40% probability, 3 points is a 93% probability, and 4 points is a 99% probability of septic arthritis. Limitations of the criteria include the inability to rule out septic arthritis at low (or zero) scores, the original study being a retrospective review, the applicability only to the hip joint, and the lower reliability in late-presenting patients.
[https://www.mdcalc.com/calc/1817/kocher-criteria-septic-arthritis#when-to-use]
Imaging
Plain X-ray: Can help to rule out fracture, slipped capital femoral epiphysis, osteonecrosis, or bone lesions.
X-rays may also help to identify an injury in a long bone rather than a joint.
Ultrasound: The most sensitive modality for detecting a hip effusion. It does not distinguish septic arthritis from transient synovitis, but is a crucial decision-making tool.
MRI (Magnetic Resonance Imaging): Reserved for cases with diagnostic uncertainty or concern for osteomyelitis.

SCFE of left femur (right on image)

Ostenecrosis of right femur (right on image)
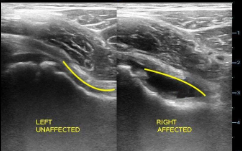
Ultrasound of Hip without (left) and with effusion (right)
Arthrocentesis
Gold standard for diagnosis.
Once the joint is identified, commonly the hip or knee, proceed with aspiration (with or without ultrasound guidance).
Synovial fluid analysis (WBC, Gram stain, Culture) is essential:
≥50,000 WBC/mm with >90% Polymorphonuclear lymphocytes strongly suggests septic arthritis.
Lower counts may still be infectious in young children or immunocompromised hosts.
In endemic areas, consider adding Polymerase chain reaction testing of synovial fluids for Lyme Disease. Synovial fluid analysis for Lyme disease will usually reveal an inflammatory effusion with ~25,000-50,000 WBC/mm with a neutrophil predominance. The fluid may appear yellow, cloudy, blood-tinged, or even slightly green.
Younger children will often require sedation to facilitate hip aspiration and often another sub-specialist available to perform the procedure (Orthopedic Surgery, Interventional Radiology, etc). This may vary by site and there may be other special considerations for rural/critical access hospitals. It is especially important to be prudent and obtain and send synovial fluid cultures for this reason when tapping a joint.
Management and Treatment
Transient Synovitis
Non-steroidal anti-inflammatories (NSAIDs) are the first-line treatment. Clinical improvement after a single dose is reassuring and further testing with labs and evaluation for septic arthritis may then be unnecessary.
If obtaining labs, consider a trial of intravenous ketorolac, which can show significant improvement
Rest and observation – outpatient follow-up with clear return precautions and around-the-clock NSAIDs for 1-2 days.
If the child still won’t walk, they may require admission for further work up and pain management.
Tips for walking trial after NSAID challenge: Pick the child up and place them a short distance from their caregiver to see if they will walk toward them. One may also try to motivate children to walk similarly with stickers, toys, or a popsicle.
No role for antibiotics or surgery.
Septic Arthritis
Immediate orthopedics consult – surgical washout is often required.
Empiric intravenous antibiotics targeting Staphylococcus aureus, including MRSA if community prevalence is high.
For non-severe infections, considerations for antibiotics can include cefazolin, oxacillin, nafcillin, or clindamycin. For more severe infections, treatment with vancomycin PLUS cefazolin or nafcillin or oxacillin is recommended
Supportive care – fluids, antipyresis, and analgesia as needed.
Lyme Arthritis
If a diagnosis of lyme arthritis is made or is suspected prior to synovial fluid analysis or cultures, patients can be admitted and treated empirically.
Treatment entails a 28 day course of an oral antibiotic (amoxicillin or cefuroxime for children <8 years old, or doxycycline for children >8 years old)
Historically, doxycycline was avoided in children <8 years old due to concern for tooth staining. Newer evidence suggests there is no increased tooth staining in children <8 years old. However, when considering treating a child <8 years old, consider an alternative or consult an Infectious Diseases specialist.
If intravenous antibiotics are required (e.g., for patients with carditis, neurologic involvement, or Lyme arthritis not responding to oral antibiotics), patients can be treated with ceftriaxone.
Clinical Pearls
Septic arthritis is a time-sensitive emergency; delay in diagnosis can lead to permanent joint damage within 24–48 hours.
Transient synovitis is far more common (40–50% of atraumatic limps), but the clinician must actively exclude infection if the patient does not show improvement (still unable to walk) after trial of NSAIDs.
Ultrasound is indispensable in early emergency department (ED) evaluation, specifically if the hip joint is the concern.
Kocher criteria are helpful but imperfect—use as part of the clinical gestalt, not a binary rule.
Always consider non-musculoskeletal mimics: psoas abscess, appendicitis, testicular torsion, malignancy (e.g., leukemia), etc.
Discharge instructions should include careful return precautions: if limp returns and is recurrent or does not improve it is important to have follow up with primary care provider and/or return to ED for consideration of other pathologies.
Conclusion
Distinguishing between septic arthritis and transient synovitis in the ED requires a careful history, systematic examination, and judicious use of diagnostics. The stakes are high. While transient synovitis is benign and self-limited, septic arthritis requires rapid intervention to preserve joint function and prevent systemic complications. Emergency providers must maintain vigilance, use ultrasound liberally, and collaborate closely with orthopedic colleagues when suspicion for septic arthritis arises.
Author: James Joseph, MD is a fourth-year emergency medicine resident at Brown Emergency Medicine.
Faculty Reviewer: Meghan Beucher, is an Assistant Professor of Emergency Medicine and Pediatrics at The Warren Alpert School of Medicine at Brown University
References
Singer JI. The cause of gait disturbance in 425 pediatric patients. Pediatr Emerg Care. 1985;1(1):7-10. doi:10.1097/00006565-198503000-00003
Lázaro Carreño MI, Fraile Currius R, García Clemente A. Non-traumatic limping in Paediatric Emergencies: Epidemiology, evaluation and results. Rev Esp Cir Ortop Traumatol (Engl Ed). 2018;62(2):127-133. doi:10.1016/j.recot.2017.10.004
Fischer SU, Beattie TF. The limping child: epidemiology, assessment and outcome. J Bone Joint Surg Br. 1999;81(6):1029-1034. doi:10.1302/0301-620x.81b6.9607
Moumile K, Merckx J, Glorion C, Pouliquen JC, Berche P, Ferroni A. Bacterial aetiology of acute osteoarticular infections in children. Acta Paediatr. 2005;94(4):419-422. doi:10.1111/j.1651-2227.2005.tb01911.x